Abstract
Hydatid disease is an endemic anthropozoonosis and is commonly caused by the tapeworm Echinococcus Granulosus.It is endemic in sheep- and cattle-raising regions, seen mainly in Mediterranean countries including Turkey.Echinococcal involvement of the breast is extremely rare, even in endemic countries. We present a 66-year-old female patient with hydatid cyst who presented with the complaint of a mass in the right breast.
Keywords :
cyst
, breast
, echinococcosis granulosus
Turkish Abstract
Kist hidatik Ecinococcus Granulosus ile bulaşan bir hastalıktır.Endemik bölgelerde, özellikle hayvanlarla teması olanlarda yaygındır.Meme kist hidatiği endemik bölgelerde bile çok nadirdir.Memeye sekonder yerleşim gösterebildiği gibi, primerde yerleşimde gösterebilir.Kliniğimize memede kitle nedeniyle başvuran 66 yaşındaki kadın hastamızı sunduk.
Turkish Keywords :
, meme
, kist
, ekinokokus granulozus
Introduction
Human hydatid cyst or cystic echinococcosis is a life-threatening zoonotic disease that occurs in most countries worldwide and is recognized as a major public health problem1. It particularly affects developing countries. The prevalence of hydatid disease is estimated to be 0.005%; the incidence of the disease is 2-12 per 100,000 persons. In Turkey, the incidence of hydatid cysts is 14 per 100 persons 2. Hydatid cysts mainly affect the liver (67%). The route of dissemination is most commonly through blood circulation and secondly through the lymphatic duct. Hydatid cysts may grow in almost every organ of the body, with the liver and lung being the most frequently targeted organs. However, the cyst tends to appear in different and sometimes unusual body sites. A hydatid cyst in the breast is very rare; reported incidence in the breast is 0.27%. Patients present with unilateral, painless, slowly growing lumps in the breast mimicking breast neoplasm clinically and they are most common in women between the ages of 30 and 503. In most cases they are discovered accidentally during a routine ultrasound or mammography. Surgical approaches remain the gold standard for diagnosis and treatment. We present a 66-year-old female patient with a hydatid cyst who presented with the complaint of a mass in the right breast.
Case Report
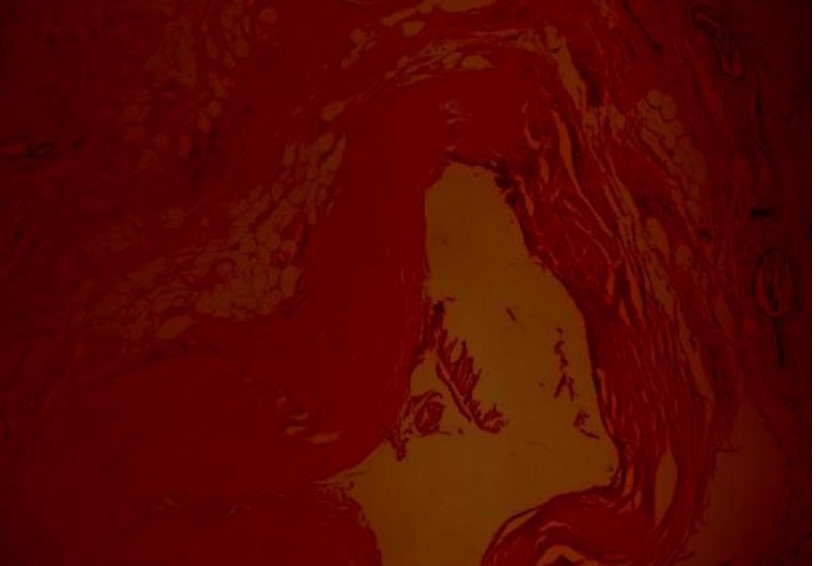
A 66-year-old female patient was admitted to our outpatient clinic due to a mass in her right breast for about one year. Breast examination by palpation revealed one discrete mass in the upper outer quadrant of the right breast, measuring approximately 3×2 cm, mobile and well circumscribed. The mammogram revealed a large, smooth-walled, well-defined opacity in the upper outer quadrant of the right breast, measuring 32×25 mm (Figure-1). In the breast ultrasonography (USG), a heterogeneous, hypo-anechoic, well-defined lesion (approximately 31×19 mm) at 10 o’clock in the right breast was seen. Fine needle aspiration cytology was performed. In the histopathology of the resected specimen, monolayered benign epithelial cells were mixed with myoepithelial cells. For a definitive diagnosis, excisional biopsy is recommended. On the right side, a periareolar incision was made and the tissues between the subcutaneous adipose and mammary gland capsule were sharply separated until the surface of the mass was reached. The mass, together with part of its surrounding normal glands and adipose tissue, were completely removed. After one day of follow-up, she was discharged without any complication. Histopathological studies confirmed the diagnosis of hydatid cyst. Medical drugs were not used for the hydatid cyst (Figure 2-4). After two years, abdomen and thorax computed tomography (CT) and mammography were performed and no cyst was detected. We considered this case as an isolated primary hydatid cyst of the breast. Following the operation, an IHA test conducted for echinococcus was negative. Thorax and abdomen BT revealed no other lesion consistent with the hydatid cyst.
Discussion
Hydatid cyst of the breast is seen very rarely even in the regions where the disease is endemic. Parasites usually spread to the visceral organs via the blood or lymphatic system. Rupture of a hydatid cyst of the liver is secondary to blunt abdominal trauma or iatrogenic trauma and can lead to the spread of contents to the secondary biliary tract and afterwards to the breast4,5.
The diagnosis of breast hydatid cyst is made using imaging techniques such as USG, CT, or magnetic resonance imaging (MRI), combined with case history. Serology tests can be used in addition. Mammography shows a homogeneous smooth circumscribed oval lesion. The imaging features of hydatid cyst are nonspecific. The lesion is usually seen as a circumscribed mass. The differential diagnosis includes cyst, fibroadenoma, phyllodes tumor, and circumscribed carcinoma. USG of the breast shows a well-defined, multicystic mass with layering low level internal echoes. It is difficult to detect the mass by USG or mammogram. In our case, the diagnosis could not be made by USG or mammogram6.
In MRI, the capsular wall of the mass was smoothed and moderately thickened4. There were internally scattered, mostly circumferential oriented small loculations separated by thin septations. According to the indirect hemagglutination test results, hydatid cyst of the liver is positive for over 80% but for a typical localization of cyst percentages can be lower; herein the test result for hydatid cyst of the breast was negative. Fine needle aspiration biopsy can be performed to diagnose hydatid cyst7. In our case, the aspiration biopsy did not detect cysts. Open surgical procedures such as cystectomy are the basis of the treatment of hydatid cyst of the breast6. The number of eosinophils in the peripheral blood can increase about half with hydatid cysts, but in this case the eosinophil count was within the normal range8.
Conclusion
Hydatid cyst of the breast is very uncommon. It is very challenging to differentiate it from other tumoral lesions of the breast. However, it should be included in the differential diagnosis of breast lumps for patients living in endemic areas. Surgical approaches are the main treatment and total cystectomy should be performed.
Informed Consent
From the Patient
References
- Şenlik B. Echinococcus türlerinin gelişmeleri. Echinococcosis Hidatidoloji D.2004;1:31-42.
- Yüksel M, Kalaycı G. Akciğer Kist hidatiğinin cerrahi tedavisi. Göğüs Cerrahisi. İstanbul: Bilmedya grup. 2001;1;647-658.
- Uncu H, Erekul S. Hydatid cyst of the breast. Acta Chir Belg 2007; 107(5): 570-571.
- Köksal H, Aslan N, Akın N. İzole meme kist hidatik olgusu .Genel Tıp Derg. 2011;21(3): 111- 113.
- Ali A, Aldhilan A, Makanjuola D, Abdulmohsen A. Preoperative diagnosis of hydatid cyst of the breast: a case report. Pan Afr Med J. 2013; 14: 99.
- Yaghan RJ. Hydatid Disease Of The Breast: A Case Report And Literature Review. Am. J. Trop. Med. Hyg .1999;61: 714–715.
- Dirican A, Unal B, Kayaalp C, Kirimlioglu V. Subcutaneous hydatid cysts occurring in the palm and thigh: two case reports. J Med Case Reports 2008;2: 273.
- Rai LCSP, Panda BBN, Ganguly CD, Bharadwaj LCR. PulmonaryHydatid: Diagnosis and Response to Hypertonic Saline Irrigation and Albendazole. MJAFI .2005; 61:69-12.
|