Abstract
Many chemotherapeutic agents are defined with their neurotoxic effects. And also, the peripheral nerve entrapments are one of the major disorders in the neurosurgery clinics and cause of neuropathy. The aim of both neurotoxicity and nerve entrapment?s urgent treatment protocol is full recovery but the treatment modalities are different.
Case description: In this report, the authors present rare case of a peroneal nerve entrapment as a complication of chemotherapeutic agents induced weight loss. A 61-year old male patient with pancreas adenocarsinoma and multiple liver metastases presented with right foot drop. A clinical diagnosis of peroneal nerve entrapment was confirmed by electrophysiological study. He underwent urgent decompressive surgery for common peroneal nerve. A good neurological recovery was achieved on postoperative 1st day and he was neurologically intact at the postoperative 6th month.
Conclusion: We believe that it is important to decide surgery for the treatment of a neuropathy irrespective of the etiology so; the differential diagnosis must have been done properly.
Keywords :
peroneal nerve
, entrapment
, gemcitabine
, 5- fluorouracil
, weight loss
Turkish Abstract
Birçok kemoterapötik ajanın nörotoksik etkileri vardır. Bununla birlikte, periferik sinir tuzaklanması nöroşirürji kliniklerindeki en önemli bozukluklardan bir olup nöropatinin bir başka nedenidir. Hem nörotoksisitenin hem de sinir tuzaklanmasında acil tedavi protokolünün amacı tam iyileşmedir.
Bu yazıda, kemoterapötik ajanların neden olduğu ani kilo kaybının nadir bir komplikasyonu olarak görülen bir peroneal sinir tuzaklanması olgusu sunuldu. Pankreas adenokarsinomu ve çok sayıda karaciğer metastazı olan 61 yaşında erkek hasta kliniğimize sağ ayak kuvvet kaybı ile başvurdu. Elektrofizyolojik çalışma ile Peroneal sinir sıkışmasının klinik teşhisi konuldu. Peroneal sinir tuzaklanması için acil dekompresif cerrahi yapıldı. Postoperatif 1. günde iyi bir nörolojik iyileşme sağlanırken postoperatif 6. ayda hasta nörolojik olarak düzeldi.
Biz etiyolojisine bakılmaksızın periferik sinir sıkışlığının tedavisinde cerrahi tedavinin önemli olduğuna inanıyoruz.
Turkish Keywords :
, peroneal sinir
, tuzaklanma
, gemcitabine
, 5- fluorouracil
, kilo kaybı
Introduction
Peripheral nerve dysfunctions (motor weakness, sensorial deficits, neuropathic pain, etc.) that were caused by entrapment or neural toxicity, need emergent surgeries. Peripheral nerves may be entrapped along their course either acutely or as a part of a chronic process. However neurotoxic side effects of the medicines may also cause nerve dysfunction.1 When clinical findings are suggestive of entrapment and/or neural toxicity, the diagnosis must be confirmed with electrophysiological studies.2
After the nerve injury, neurons can regenerate by axonal sprouting, and functional synapses can form, leaving the patient with some recovery of sensation or function. Functional recovery after serious nerve injuries is poor and resulting neuropathic pain or permanent deficits.3 The aim of the urgent treatment for nerve lesion caused by either neurotoxicity or entrapment is complete neurological improvement.
We present a patient with pancreas adenocarsinoma who had multiple liver metastases and developed peroneal nerve entrapment during the chemotherapy. The electrophysiological and surgical features of the patient were documented and discussed with the literature.
Case Report
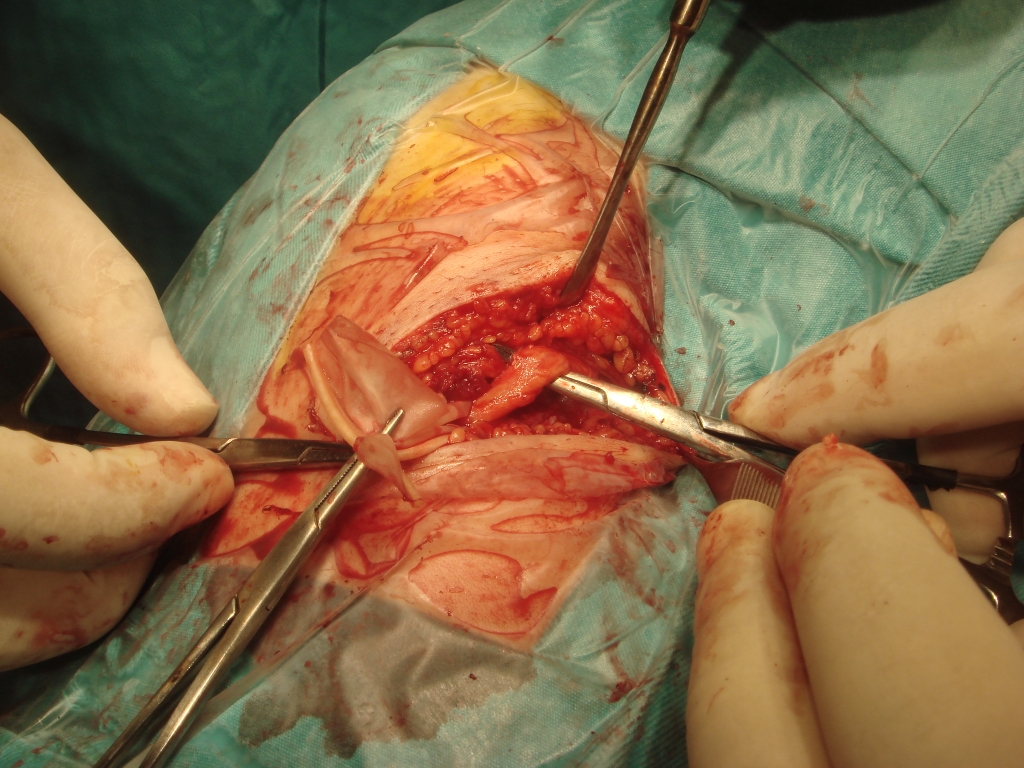
A 61-year old male patient, who had a history of severe weight loss of (24 kg) during the last two months, was diagnosed a pancreas adenocarcinoma with multiple liver metastases. After histopathological confirmation, the patient underwent chemotherapy with Gemcitabine (GMC) 1900 mg/day and 5- fluorouracil (5-FU) 750 mg/day, continuous infusion. He had also sudden weight loss due to chemotherapy protocol. Following the fourth session of the chemotherapy, he had a sudden right foot drop. There was neither history of trauma or surgery to the lower limb, nor history of spinal disorder. Neurological examination revealed right L4 and L5 hypoesthesia, 1/5 motor function at dorsoflexion of his right foot. Magnetic resonance imaging of lumbar spine was normal. A right common peroneal nerve entrapment was diagnosed by electrophysiological study. The patient underwent urgent decompressive surgery for common peroneal nerve. There was not any fibrous band or scar tissue which caused entrapment around the peroneal nerve, but the nerve was deformed under peroneus longus muscle and had softness like a jelly. External neurolysis performed along the axis of the neural sheath (Figure 1).4
A good neurological recovery was achieved on postoperative 1st day and he had 3/5 motor function at dorsoflexion of foot. Patient underwent early physical therapy with active assistive exercises (4 to 10 times a day) in bed for 7 days and was discharged with home program of active and progressive resistive exercises. At the postoperative 6th month, the patient was neurologically intact. But, he died at the postoperative 8th month because of the complications of primary disease.
Discussion
Common peroneal nerve is usually compressed around the fibular head or may be injured by direct trauma. The knee is also mobile and causes a continuous mechanical irritation on the nerve sheet. It is usually attributed to an excessively thick fibrous arch that narrows the tunnel which the nerve passes.
Therefore, the evaluation of peroneal nerve entrapment is made on the basis of a combination of clinical and electrophysiological findings. In our case, although the preoperative electrophysiological tests showed the peroneal nerve entrapment, the nerve was like a jelly and we could not find any clue of nerve entrapment during the surgery.
Not only are the target tissue but the normal tissue and organs affected by chemotherapeutic treatment of carcinoma and metastases.5 5-FU is a pyrimidine analogue and usually combined with radiotherapy. Today, adjuvant therapy for pancreas adenocarcinoma with radiation and 5-FU has become a standard in practice.2 The side effects of 5-FU include nausea, vomiting and diarrhea, leucopenia and thrombocytopenia, hand-foot syndrome, mucositis and cardotoxicity.6, 7 Neurotoxicity occurs only in 5% of all cases and mostly involves an acute cerebellar syndrome with loss of coordination, nystagmus or bilateral oculomotor nerve palsy, and generalized motor weakness.8 5-FU’s peripheral neurotoxicity has rarely been discussed.9 Stein et al. reported a rectal and sigmoid cancer patient with a peripheral neuropathy caused by a combination of 5-FU with levamisole.8 Van Laarhoven et al. described a complication with 5-FU and leucovorin without previous radiotherapy.10 Werbrouck et al. discussed the occurrence of the sensorimotor neuropathy due to 5-FU and radiotherapy of the pelvis.11 The patient underwent adjuvant chemotherapy with 5- fluorouracil without radiotherapy at the oncology department.
The etiology of the neurotoxicity is probably multifactorial and incompletely understood. Both the drugs and their catabolites are accused for toxicity. The possible mechanisms of neurotoxic effects of 5-FU on the neural tissue are direct neurotoxic effect, induced thiamine deficiency, and inhibition of Krebs cyclus2. And dihydropyrimidine dehydrogenase deficiency also plays an important role at the neurotoxicity.3
However, GMC is the other chemotherapeutic agent. Gemcitabine is a new cytidine analogue and a chemotherapeutic agent for pancreas adenocarcinoma.9 The most common ( ≥20% ) adverse reactions of single-agent GMC are nausea/vomiting, anemia, increased ALT, increased AST, neutropenia, increased alkaline phosphatase, proteinuria, fever, hematuria, rash, thrombocytopenia, dyspnea, and edema. Capuchino et al. have also reported WHO grade 1-2 neuropathies after GMC treatment.12 In the presented case, motor neuropathy occurrence is remarkable after the 4th session of treatment with 5-FU and GMC. There was not any statement about cessation of GMC and resolution of the symptoms.
One of the important findings was sudden weight loss. And also, in our case, the patient had a remarkable chemotherapeutic agent-induced sudden weight loss. Veerman et al. suggested that continuous infusion of Gemcitabine has provoked weight loss.1 In the literature, there are case reports about peroneal entrapment secondary to anorexia nervosa.13-16 Sprofkin decided that anorexia nervosa may cause changes in the subcutaneous tissues that led to adhesions and perineural fibrosis.17 However, relative immobility and prolonged period of inertia may thus have contributed the symptoms of the patients. And also, partial refeeding and resumption of activity diets may contribute resolution of the symptoms.16
We reviewed the literature about GMC-induced sudden weight loss with peroneal nerve entrapment. It is difficult to find a predisposing factor for peripheral nerve neuropathy because of cancer patients’ complexity (sudden weight loss, multi-chemotherapeutic agents, radiotherapy, etc.) as in our case. Faster evaluation and early surgery are still effective for peripheral entrapments but neurotoxic effects can recover by the cessations of the chemotherapeutics agents.4 5-FU can provoke peripheral neuropathy but there are not more proven and faithful studies about the neurotoxic effects of GMC in the literature. This is the first case report of GMC induced sudden weight loss with secondary peripheral nerve entrapment.
Conclusion
To our knowledge, such a case has not been previously reported. 5-FU, GMC or sudden weight loss can be accused as a predisposing factor. Furthermore, combinations of chematherapatic agents are necessary and show considerable efficacy in patients with inoperable or metastatic pancreatic cancer. Surgery is essential for peroneal nerve entrapment.
References
- Veerman G, et al. Antitumor activity of prolonged as compared with bolus administration of 2',2'-difluorodeoxycytidine in vivo against murine colon tumors. Cancer Chemother Pharmacol. 38(4): 335-342, 1996
- Van Kuilenburg AB. Dihydropyrimidine dehydrogenase and the efficacy and toxicity of 5-fluorouracil. European J Cancer. 40: 939–950, 2004
- Mark S, Greenberg MD. Injury classification system. In: Handbook of Neurosurgery. 3rd edition. 1994, pp 411-412.
- Saif MW, et al. Peripheral neuropathy associated with weekly oral 5-fluorouracil, leucovorin and eniluracil. Anti-cancer Drugs. 12: 525–531, 2001
- Broekx S, Weyns F. External neurolysis as a treatment for foot drop secondary to weight loss: a retrospective analysis of 200 cases. Acta Neurochir (wien). 160(9):1847-1856, 2018
- Kuropkat C, et al. Severe cardiotoxicity during 5-fluorouracil chemotherapy: a case and literature report. Am J Clin Oncol. 22(5): 466-470, 1999
- Sucker C, et al. Neurotoxicity of 5-fluorouracil. Deutsche medizinische Wochenschrift. 127: 2011–2014, 2002
- Stein ME, et al. A rare event of 5-fluorouracil-associated peripheral neuropathy: a report of two patients. Am J Clin Oncol. 21: 248–249, 1998
- Endlicher E, et al. Irinotecan plus Gemcitabine and 5-Fluorouracil in Advanced Pancreatic Cancer: A Phase II Study. Oncology. 72: 279–284, 2007
- Van Laarhoven HW, et al. 5-FU-induced peripheral neuropathy: a rare complication of a wellknown drug. Anticancer Research. 23: 647–648, 2003
- Werbrouck BF, Pauwels WJ, De Bleecker JL. A case of 5-fluorouracil-induced peripheral neuropathy. Clin Toxicol (Phila). 46(3): 264-266, 2008
- Capuchino I, Suarez ER, del Giglio A. A phase I study of gemcitabine combined with vinblastine in patients with solid tumors. Tumori. 89(4): 397-399, 2003
- Constanty A, et al. Peroneal nerve palsy in anorexia nervosa: three cases. Arch Pediatr. 7: 316–317, 2000
- Kershenbaum A, et al. Bilateral foot-drop in a patient with anorexia nervosa. Int J Eat Disord. 22: 335-337, 1997
- Lutte I, et al. Peroneal nerve palsy in anorexia nervosa. Acta Neurol Belg. 97: 251–254, 1997
- Sevinç TT, et al. Bilateral superficial peroneal nerve entrapment secondary to anorexia nervosa: a case report. J Brachial Plex Peripher Nerve Inj. 3(1): 12, 2008
- Weyns FJ, et al. Foot drop as a complication of weight loss after bariatric surgery: is it preventable? Obes Surg. 17(9): 1209–1212, 2007
Information Presentation
14th Congress of Balkan Military Medical Congress, Bulgaria, May 10-14, 2009
|