Abstract
Aortic dissection is a life threatening condition that requires an early diagnosis to prevent mortality. Typically it presents with acute chest, back, and tearing abdominal pain. Early diagnosis is critical because there is 1-2 % mortality per hour after symptom onset in those whom the problem goes unrecognized. . It can be seen with different clinical findings without pain. Left-sided neurologic deficits, dyspnea, syncope and bilateral lower extremity deficits are the most common symptoms. Additionally in the presence of ischemia involving multiple organs aortic dissection should be considered
We report a two cases of painless huge fusiform aortic aneurysm and dissection. One of them complicated by transient ischemic stroke, which was treated with conservative approach, and three year follow –up without any complication. Other report was applying to the our emergency service with atypical presentation worsening dyspnea and treated successfully surgical operation.
Aortic dissection is a cardiac emergency that requires rapid diagnosis and treatment .A painless presentation is a rare occurrence in about 6,4-17 % of cases and this linked to poor outcomes. It should be remembered that delays in diagnosis can lead to catastrophic consequences.
Keywords :
Aortic dissection
, ischemic stroke
, aortic aneurysm
Turkish Abstract
Aort diseksiyonu, mortaliteyi önlemek için erken tanı gerektiren, yaşamı tehdit eden kardiyak acildir. Tipik olarak ani başlayan göğüs, sırt ve yırtıcı tarzda karın ağrısı ile kendini gösterir. Erken teşhis kritiktir çünkü sorunun farkına varılmadığında semptom başlangıcından sonra saatte % 1-2 mortalite oranı vardır. Ağrısız farklı klinik bulgularla görülebilmektedir. Sol taraflı nörolojik defisit, dispne, senkop ve bilateral alt ekstremite defisitleri en sık görülen semptomlardır. Ek olarak, çok sayıda organı içeren iskemi varlığında aort diseksiyonundan şüphelenilmelidir.
İki adet ağrısız büyük fuziform aort anevrizması ve diseksiyonu olgusunu sunuyoruz. Bunlardan biri konservatif yaklaşımla gidilen, geçici iskemik inmeyle başvuran ve sonrasında herhangi bir komplikasyon olmaksızın üç yıl takip edilen hasta, diğer hastamız ise atipik semptomla, kötüleşen dispne ile acil servisimize gelen ve başarılı cerrahi girişimle tedavi edilen vakadır.
Aort diseksiyonu, hızlı tanı ve tedavi gerektiren kardiyak acildir. Ağrısız bir prezentasyon, hastaların yaklaşık% 6,4-17' sinde görülebilen nadir bir durumdur ve kötü sonuçlarla ilişkilidir. Tanıdaki gecikmelerin mortalitede artışa yol açabileceği unutulmamalıdır.
Turkish Keywords :
, Aort diseksiyonu
, iskemik stroke
, aort anevrizması
Introduction
Aortic dissection (AD) is a life threatening emergency leading to poor outcomes in the absence of early diagnosis and treatment. The risk of mortality can be reduced by early and rapid diagnosis .Timely diagnosis and triage is critical because as every hour of delay 1% increase in mortality 1. According to the report estimates incidence of AD, 3 to 4 cases for per 100.000 people 2. AD can lead to ischemia in extremities and multiple organs (arms or legs 20%, kidney 15 %, myocardium 10%, brain 5%, mesentery or spinal cords 3%), cardiac tamponade, shock and death 3. Painless AD is a rare occurrence in about 6,4-17 % of cases and this linked to poor outcomes 4-5. Herein we report a two cases of painless huge fusiform aortic aneurysm and dissection. One of them complicated by transient ischemic stroke, which was treated with conservative approach, and three year follow –up without any complication. Other report was applying to the our emergency service with atypical presentation worsening dyspnea and treated successfully surgical operation.
Case Report
Case report-1
A 74-year- old male patient applied to our emergency department with complaints of numbness and weakness in the left arm and leg, which started suddenly. The patient had a by-pass operation 2 years ago and history of hypertension for 10 years. Upon arrival, the patient did not have chest pain. His right arm blood pressure was 120/70 mm/hg and left arm was 145/95 mm/hg, heart rate 75/beats per minute and rhythmic, respiration 24 times per minute, oxygen saturation 97% on room air, and his fewer was measured 36,7. No ischemic findings ,ST-T changes, or atrial fibrillation was detected in the electrocardiography. Laboratory results revealed elevated white blood cell count (13,0x109/L; 4,0-10,0x109/L) ,creatinin (1,4 mg/dl; 0,6-1,2 mg/dl), D-Dimer (2,3 μg/mL; 400 <μg/mL) and blood urea nitrogen level (38 mg/dl 10-16 mg/dl). Other biochemical tests, protrombin time and international normalized ratio (INR) was normal. Cardiac auscultation was no aortic regurgitation murmur and pulses were normal and symmetric in all 4 extremities. His lungs were clear to auscultation.
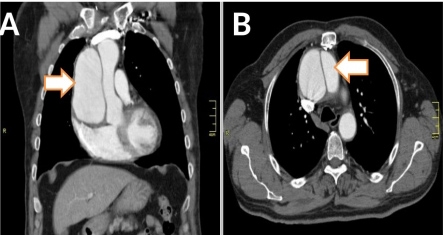
The patient was evaluated by contrast-enhanced thorax CT after the increase the cardiothoracic ration and the widening of mediastinum was seen in the chest x-ray . There was a huge fusiform aortic aneurysm (77 millimeter) and Stanford type A dissection extending in the 110 millimeter segment from to aortic root (figure 1A-B).
The patient was followed up in the intensive care unit. It was decided to follow medical therapy, because vital sings was stable and there was no chest pain. Furthermore, we concluded that the risk of re-operation was high.
The patient was removed in the intensive care unit after 5 days and low dose warfarin treatment was initiated (target INR 1,6-2,5). At the end of the 10th day, medical treatment was arranged and patient was discharged without any neurological deficit. In the follow-up 3 years did not develop any complications. The patient was the followed INR levels every 20 days, echocardiographic examination every 3 mounts and chest CT every 6 mounts. There was no increase in aortic diameter during this period.
Case report-2
A 42 year women admitted to our clinic with complaints of dyspnea, anorexia, weakness and insomnia during the last week .She had the history of rheumatic valve disease for long years. The patient who had no hypertension or pregnancy and did not describe any pain. She has not been in control for 2 years and she did not used any medicine. Her blood pressure was right arm 110/70 mm/hg and left arm 135/85 mm/hg, heart rate 98 /beats minute and oxygen saturation 92 on room air. Cardiac examination revealed that pronounced systolic ejection murmur and her lungs auscultation crepitan rales at 1/3 basal levels. All pulses were normal and palpable. Her ECG was sinus tachycardia without any ischemic changes. 2 D echocardiography showed advanced mitral regurgitation with rheumatic mitral valve, dilatation of the aortic root and arch with suspicions flap appearance in the ascending aorta and moderate aortic insufficiency. Left ventricular dilatation (LVD d 6,0 cm, LVS d 4,9 cm) and hypertrophy was found but ejection fraction was normally (LVEF 63 %).
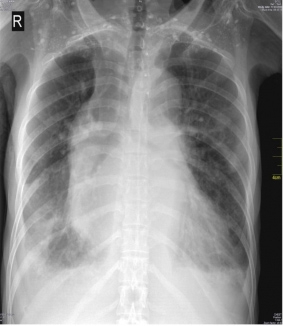
Chest X-ray showed increased cardiothoracic ration and over the mid and lower lung fields with fluid appearance like heart failure (figure 2).
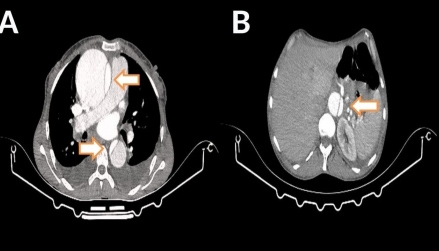
Her blood tests revealed mildly elevated troponin (0,8 ug/ml; < 0,02 ug/ml ) and CRP levels ( 25 mg/L; < 0,5mg/L). Other parameters were normal. The patient was evaluated by contrast-enhanced thorax CT and aortic diameter was found 79 millimeters and intimal flap extending right iliac artery from to ascending aorta compatible with Stanford type A AD ( figure 3 A-B). The patient underwent the operation of aortic root reconstruction (Bentall’s procedure) with mechanical prosthetic aortic valve and mitral valve repair surgery successfully.
Discussion
AD classified as based on the starting time of complaints as acute if less than 2 weeks of onset of symptoms and chronic if the diagnosis is made later6. Additionally Stanford classification, into type A that involves the ascending aorta and may progress to involve the arc and thoraco-abdominal part. Type B dissection starts after the left subclavian artery without involvement of ascending aorta.. Emergency surgery considered in type A and medical treatment is generally recommended in type B dissection.
Type A aortic dissection is a life-threatening emergency with mortality rates > 50% in first 24 hours, increasing up to 75% within 2 weeks of the event 2-3. Early surgical intervention in patients with type A aortic dissection decreases mortality7-8. Additionally painless AD is more prevalent among patients suffering from type A dissection than type B dissection5.
The most common symptoms in AD is sudden onset of severe chest pain in type A and abdominal pain in type B dissection. In addition various symptoms such as syncope, dyspnea, left and right sided deficits, bilateral lower extremity deficits, loss of consciousness, amnesia, and paralysis can be seen. Also some patients are asymptomatic. Neurologic deficits have been associated with 17 % to 40 % cases of AD. The diagnosis of this patients is more difficult and it can be delayed. The cause of painless AD is unclear. There are many different hypotheses have been suggested to explain the absence of pain. Cerebral ischemia can change the pain threshold and aortic aneurysm, diabetes mellitus, advanced age, previous surgery may have damaged innervation to the aorta.
Misdiagnosis in painless AD presenting with neurological complaints may lead to fatal results such as thrombolytic therapy. In AD, the early mortality rate of patients given thrombolysis is very high can be up to 70 % 9. Therefore, it is very important to make a fast and accurate diagnosis.
After we decided for the patient not to operate, low dose warfarin treatment started to prevent partial thrombosis of the false lumen. Some physicians suppose that warfarin increase the risk of aortic rupture accelerates progression of dissection10. We have not encountered the use of warfarin therapy for type A dissection in the literature.
References
- Braverman AC. Acute aortic dissection clinician update. Circ 2010;122(2):184-88.
- LeMaire SA and Russell L. Epidemiology of thoracic aortic dissection. Nat Rev Cardiol 2011- Rewiev 8(2),103-13.
- Meszaros I, Morocz J, Szlavi J,et al. Epidemiology and clinicopathology of aortic dissection. A population-based longitudinal study over 27 years. Chest 2000;117:71–78.
- Hagan PG, Nienaber CA, Isselbacher EM ,et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA 2000;283:97-03.
- Matsuo H. Clinical significance and impact of “painless” acute aortic dissection. Circ J 2011;75:47-8.
- Lachat M, Criado FJ, Veith FJ. The case for anticoagulation in patients with acute type B aortic dissection. J Endovasc Ther 2008;15-52-3.
- Thrumurthy SG, Karthikesalingam A, Patterson BO, et al. The diagnosis and management of aortic dissection. BMJ 2012;344:d8290
- Mehta RH, Suzuki T, Hagan PG, et al. International Registry of Acute Aortic Dissection (IRAD) Investigators. Predicting death in patients with acute type A aortic dissection. Circ 2002;105:200–06
- Kamp TJ, Goldschmidt-Clermont PJ, et al. Myocardial infraction, aortic dissection, and thrombolytic therapy. Am Heart J 1994;128(6):1234-37.
- Khan IA, Nair CK. Clinical, Diagnostic, and management perspectives of aortic dissection. Chest J 2002;122(1):311-28.
|