Abstract
Choledochal cysts (CCs) are a congenital dilatation of the extrahepatic and/or intrahepatic bile duct which are commonly associated with pancreaticobiliary maljunction. Abdominal pain and recurrent attacks of acute pancreatitis due to protein plugs or stones occur in 5-30% of patients with remnant intrapancreatic choledochal cysts (IPCCs). The aim of this study was to report a case with abdominal pain of protein plugs and stones due to remnant IPCCs after incomplete prior resection. A 49-year-old female patient presented with abdominal pain on the epigastrium and right upper quadrant with intermittent fever, nausea, vomiting and weight loss that had lasted for more than six months. One and a half years prior, the patient had been diagnosed as a type I CC and undergone cyst excision with Roux-en-Y hepaticojejunostomy plus cholecystectomy at another hospital. Magnetic resonance cholangiopancreatography (MRCP) marked cytic dilatation of the extrahepatic bile duct (remnant cyst) and an intraluminal mass. Endoscopic retrograde cholangiopancreatography (ERCP) was performed and protein plugs were removed from the distal common bile duct. The symptoms were partially relieved and she had complaints repeatedly so it was decided to apply the Whipple procedure. Standard pancreaticoduodenectomy was performed. Patient?s postoperative period was uneventful and she was discharged on the 7th postoperative day.
Keywords :
Remnant Choledochal cysts
, Surgery
, Complete excision
Turkish Abstract
Koledok kistleri, ekstrahepatik ve / veya intrahepatik safra kanalının konjenital dilatasyonudur ve genellikle pankreatiko-biliyer malformasyon ile ilişkilidirler. Remnant intrapankreatik koledok kistleri olan hastaların % 5-30' unda protein tıkacı veya taşlara bağlı karın ağrısı ve akut pankreatit atakları oluşur. Bu çalışmanın amacı, yetersiz rezeksiyon sonrası rezidüel intrapankreatik koledok kistlerine bağlı protein tıkaçları ve taşları nedeniyle kronik karın ağrısı olan bir olgunun sunulmasıdır.
Kırk dokuz yaşında bayan hasta epigastriumda ve sağ üst kadranda son altı aydır olan karın ağrısı, aralıklı ateş, bulantı-kusma, kilo kaybı şikayetleriyle başvurdu. Bir buçuk yıl önce hastaya başka bir hastanede koledok kisti tanısı konularak koledok kist eksizyonu, Roux-en-Y hepatikojejunostomi ve kolesistektomi yapılmıştı. Hastanın çekilen magnetik resonans kolanjiopankreatograf (MRKP)? sinde ekstrahepatik safra kanalının distalinde kistik genişleme(remnant koledok kisti) ve intraluminal milimetrik taş ile uyumlu lezyonlar saptandı. Endoskopik retrograd kolanjiopankreatografi (ERKP) ile remnant kistik dilate koledoktan protein tıkaçları çıkarıldı. Semptomlarında kısmi rahatlama olan ve şikayetleri mükerrer kez tekrarlayan hastaya Whipple prosedürü uygulanmasına karar verildi. Hastaya standart pankreatikoduodenektomi ameliyatı yapıldı. Hastada operasyon sonrası komplikasyon gelişmedi ve hasta postoperatif 7. gün taburcu edildi.
Turkish Keywords :
, Remnant koledok kisti
, Cerrahi
, Tam eksizyon
Introduction
Choledochal cyst (CC) is a congenital dilatation of the extrahepatic and/or intrahepatic bile duct which is commonly associated with pancreaticobiliary maljunction. The incidence of CCs is higher in females, with a female to male ratio of 4:1 1. The current recommended treatment for type I CC is total cyst excision with Roux-en-Y cholangiojejunostomy 2,3. Nevertheless, this operation is particularly difficult when the cystic lesion extends deeply into the pancreas.
Abdominal pain and recurrent attacks of acute pancreatitis due to protein plugs or stones occur in 5-30% of patients with remnant intrapancreatic choledochal cysts (IPCCs) 4,5. Additionally, remnant cysts may lead to subsequent malignant transformation, with an incidence of 0.7?6 % 6.
The aim of this study was to report a case with abdominal pain of protein plugs and stones due to remnant IPCCs after incomplete prior resection.
Case Report
A 49-year-old female patient presented to our clinic with epigastric and right upper quadrant pain, anorexia, intermittent fever, nausea, vomiting and weight loss, in the last 6 months. In her history; one and a half years prior, the patient had been diagnosed with a type I bile duct cyst and had undergone cyst excision, Roux-en Y hepaticojejunostomy and cholecystectomy at another hospital. Histopathologic findings from that time showed no evidence of malignancy of choledochal cyst. On physical examination, the patient had a cachectic appearance and had a right subcostal incision. There was pain in the epigastric region with palpation. She was a well-appearing, non-jaundiced female and no evidence of hepatosplenomegally, lymphadenopathy, or masses; beside this, there was no significant finding including vital sign. Initial laboratory values included WBC of 8.300/?L, albumin of 4.7 g/dL, total bilirubin of 0.78 mg/dL, direct bilirubin of 0.45 mg/dL, AST/ALT of 41/80 IU/L, alkaline phosphatase of 198 IU/L, ?-GTP of 187 IU/L, ?-FP of 0.5 ng/mL, CEA of 0.5 ng/mL, CA 19-9 of 3.03 U/Ml. Histopathologic findings from that time showed no evidence of malignancy of bile duct cyst.
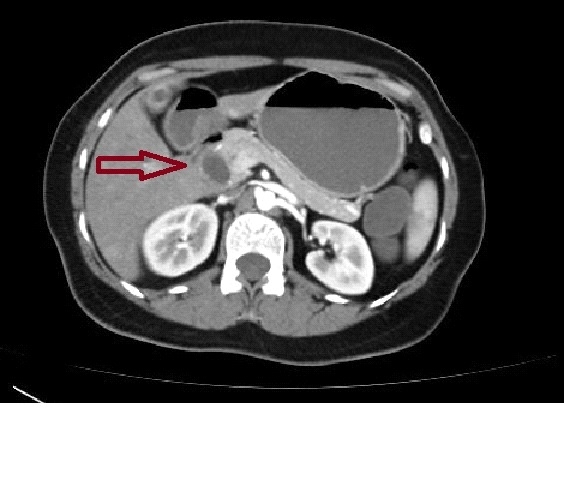
Radiologically, a cystic dilatation and intraluminal hypoechoic lesion of the extrahepatic bile duct was detected in abdominal ultrasonography (US). Abdominal tomography revealed marked cytic dilatation of the extrahepatic bile duct (remnant cyst) (Figure 1).
Magnetic resonance imaging (MRI) - MRCP marked cytic dilatation of the extrahepatic bile duct (remnant cyst) and intraluminal intensive collection (abscess) and a milimetric lesion (bile stone?) in the distal ex c bile duct (Figure 2).
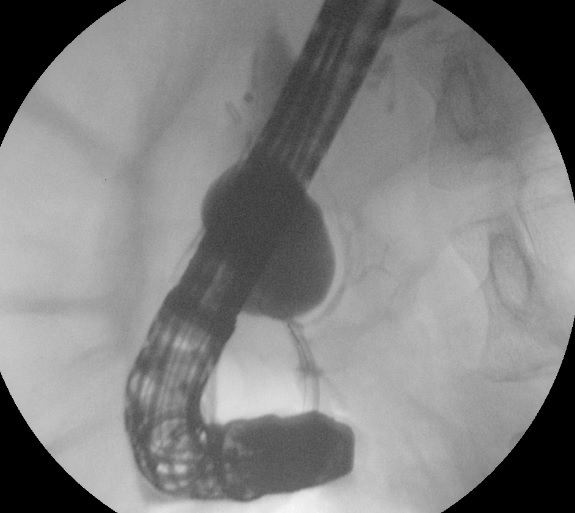
The patient was hospitalized because of abscess in the remnant bile duct cyst with accompanying severe epigastric pain and nausea. Parenteral liquid hidration and nutrition has began. Empirically broad spectrum antibiotics and analgesics were given. Despite intensive care for a week, her complaints could not be relieved so ERCP was performed and protein plugs was removed from the remnant distal common bile duct (Figure 3) and a plastic stent was inserted with the aim of drainage of the remnant cystic content.
During follow-up her complaints decreased and she was discharged to come to the control. Two weeks after her discharge, the patient was readmitted due to epigastric pain, nocturnal high fever and nausea. The stent was clogged and replaced with a new stent by ERCP. The symptoms were partially relieved after the ERCP but later her complaints repeated so it was decided to perform a Whipple procedure. After the procedure was approved by the patient, she underwent the resection of distal extrahepatic bile duct with standard pancreaticoduodenectomy. The histopathological examination for the resected specimen yielded the final diagnosis of remnant CC with no evidence of malignancy. The patient showed no postoperative complication and was discharged on the 7th postoperative day. She has been regularly followed at outpatient department with no evidence of abdominal symptoms more than one and a half years.
Discussion
The incidence of the protein plugs or stones in remnant IPCCs is not uncommon. The presence of a remnant IPCCs may lead to the formation of a dead space within the pancreas. Pancreatic secretions can be forced to move into the dead space due to the the anomalous pancreatobiliary junction (APJ) 7,8. Due to APJ, abnormal function of duodenal papilla results in backflow of intestinal secretions, that activates pancreatic enzymes in the remnant IPCCs, which may lead to infection and an increased risk of malignancy 9. Reflux of protein fluid to the remnant IPCCs dead space is the main pathogenic mechanism of stone or protein plugs formation 4,5. In a study, protein plugs or stones were detected 28-36% of remnant IPCCs excised patients with routine intra-operative endoscopy 10.
Total cyst excision is the ideal treatment of the CCs if it can be accomplished without injury. Also, if the distal excision point cannot be reached without injury to the pancreas, pancreaticoduodenectomy may be required. In our patient, stone and plugs developed in residual IPCC after partial excision and this led to symptomatic long-term pain complaints in her. In exploration, the distal surgical margin could not be achieved without injury to the pancreas, therefore pancreaticoduodenectomy was performed.
While the surgical efficacy has improved greatly, the reoperation rate has remained high and is reported to range from 30 to 37 %. 11 In one study, Xia HT et al 12 found that more than one third of patients requiring reoperation had Todani type I CCs, and about half of the patients requiring reoperation had Todani type IV CCs.
Malignant transformation risk should be kept in mind after incomplete resection of IPCCs. The incidence of metachronous carcinoma was found to be dependent on the completion of resection and this incidence was reported to be between 20% and 30% in untreated CCs from 0.7% to 11% in incomplete resections 13,14. In addition, a study showed that this risk is 1.6%, 3.9% and 11.3% after 15, 20 and 25 years after excision of the cyst. 14 Another study showed that the mean duration between incomplete cyst function and malignancy diagnosis was 140 months 14. The risk of malignancy also depends on the type of CC cyst: type 1 and 4 are higher than types 2, 3 and 5 14. In our case, no malignancy was reported in the histopathologic examination.
There is no consensus or recommendation for proper follow-up method and duration 14 . All patients with CCs require long-term follow-up for bile duct cancer, using ultrasonography and laboratory investigations including liver parameters, cancer markers [carcinoembryonic antigen (CEA), CA 19-9, CA-125] 13 applied every 6-12 months; also if necessary abdominal computed tomography (CT)scan or pancreatic endosonography or MRCP scan have been widely accepted for follow-up 13-14.
In conclusion, complications (cronic abdominal pain, pancreatitis) seem to be common with remnant IPCCs. Additionally, the risk of subsequent biliary malignancy in patients undergoing incomplete choledochal cyst excision seems to be relatively high in the long-term. For these reasons; to improve outcomes, the intrapancreatic portion of CCs should be resected completely at the time of surgical resection of the CCs.
References
- Atkinson HD, et al. Choledochal cysts in adults and their complications. HPB (Oxford). 2003; 5:105-10.
- Voyles CR, Smadja C, Shands WC, Blumgart LH. Carcinoma in choledochal cysts. Age-related incidence. Arch Surg. 1983; 118:986- 8.
- Bismuth H, Krissat J. Choledochal cystic malignancies. Ann Oncol. 1999; 10 (Suppl 4):94-8.
- Kaneko K, et al. Protein plugs cause symptoms in patients with choledochal cysts. Am J Gastroenterol. 1997;92:1018-21.
- Chiba K, Kamisawa T, Egawa N. Relapsing acute pancreatitis caused by protein plugs in a remnant choledochal cyst. J Hepatobiliary Pancreat Sci. 2010;17:729-30.
- Singham J, Yoshida EM, Scudamore CH. Choledochal cysts. Part 3 of 3: management. Can J Surg. 2010;53:51-6.
- Bhavsar MS, Vora HB, Giriyappa VH. Choledochal cysts: a review of literature. Saudi J Gastroenterol. 2012;18:230-6.
- Khandelwal C, Anand U, Kumar B, Priyadarshi RN. Diagnosis and management of choledochal cysts. Indian J Surg. 2012;74:401-6.
- Takahashi T, et al. Intraoperative endoscopy during choledochal cyst excision: extended long-term follow-up compared with recent cases. J Pediatr Surg. 2010;45:379-82.
- Xia HT, et al. Treatment and outcomes of adults with remnant intrapancreatic choledochal cysts. Surgery. 2016;159:418-25.
- Xia HT, et al. Selection of the surgical approach for reoperation of adult choledochal cysts. Gastrointest Surg. 2015; 19:290-7.
- Jab?o?ska B. Biliary cysts: etiology, diagnosis and management. World J Gastroenterol. 2012;18:4801-10.
- Ohashi T, et al. Risk of subsequent biliary malignancy in patients undergoing cyst excision for congenital choledochal cysts. J Gastroenterol Hepatol. 2013;28:243-7.
- Todani T, Tabuchi K, Watanabe Y, Kobayashi T. Carcinoma arising in the wall of congenital bile duct cysts. Cancer. 1979;44:1134-41.
|