Abstract
An obturator hernia is a rare condition accounting for 0.07-1% of the abdominal hernias; causing 0.2-1.6% of the small bowel obstructions due to the hernias. Even if they are really rare, they have the highest mortality rate of all the abdominal wall hernias reported to be between 13% and 40%. Obturator hernias are difficult cases to make a diagnosis. Surgical intervention is often delayed because of clinical and radiological diagnostic difficulty in the diagnosis. We present the case of an 83-year-old lady who presented with prolonged, over 10-12 days of intermittent small bowel obstruction admitted to the Emergency Room. Computerised tomography (CT) was taken. The cut off sign at terminal ileum just close to the right femoral canal & obturator canal was seen and the patient was taken to the operation room. The incarcerated loop in the right obturator canal and a perforation at the side of the terminal ileum was seen in the surgery. Resection and anastomosis with the repair of the hernia was done. A high suspicion for obturator hernia should be maintained in the elderly female emaciated patients with chronic disease presenting with recurrent episodes of ileus. Early diagnosis is important for better out comes.
Keywords :
Incarceration
, Hernia
, Obturator hernia
, Intestinal obstruction
Turkish Abstract
Obturator herni, tüm abdominal hernilerin %0,07-%1?ini oluşturan abdominal hernilere bağlı ince bağırsak tıkanıklıklarının da %0,2- %1,6?sına sebep olan nadir bir durumdur. Çok nadir olmalarına rağmen abdominal herniler içerisinde %13 ile %40 arasındaki oranlarla en yüksek mortaliteye sahiptirler. Obturator hernilerin tanı konulması zordur. Genellikle cerrahi tedavi, klinik ve radyolojik tanı koymadaki zorluktan dolayı gecikir. Biz burada 83 yaşında, uzamış 10-12 günlük aralıklı bağırsak tıkanması atakları şikayeti ile Acil Servis?e başvuran bir kadın hastayı sunduk. Bilgisayarlı tomografi (BT) çekildi ve terminal ileum düzeyinde sağ femoral kanal ve obturator kanal seviyesinde terminal ileuma yakın düzeyde tıkanıklık görülmesi üzerine hasta ameliyata alındı. Sağ obturator kanalda inkarsere olan terminal ileum segmenti ve bu segment lateralindeki perforasyon alanı saptandı. Rezeksiyon, anastomoz ve obturator herni onarımı yapıldı. Yaşlı, kilo kaybı ve kronik hastalıkları olan kadın hastalarda tekrarlayan ileus atakları olması durumunda obturator herni şüphesi uyanmalıdır. İyi sonuçlar için erken tanı önemlidir.
Turkish Keywords :
, İnkarserasyon
, Herni
, obturator herni
, Barsak tıkanıklığı
Introduction
An obturator hernia is a rare condition that generally requires an early surgery. Obturator hernias are difficult cases to make a diagnosis. Surgical intervention is often delayed because of clinical and radiological diagnostic difficulty in the diagnosis. Patients often present with intermittent bowel obstruction symptoms. Hernia sacs can irritate the obturator nerve within the canal, manifesting as medial thigh pain with an internal rotation of the hip at the effected side called as the Howship-Romberg Sign. Increasing speed of diagnosis through early oral and intravenous contrast enhanced computerised tomography (CT) imaging has been shown to reduce the morbidity and mortality associated with obturator hernias.
Case Report
We present the case of an 83-year-old lady who presented with prolonged, over 10-12 days of intermittent small bowel obstruction to the Emergency Room (ER). She had a prominent right low quadrant abdominal pain without any nausea or vomiting. When her previous history was taken multiple ER admissions were seen. In those admissions she described a sub-ileus clinic (Distention, difficulty in gas and passage of stool etc.) which revealed with intravenous (IV) hydration and rectal enemas. She did not have any radiological examination in those previous admissions.
In the physical examination she had an abdominal distention without any abdominal surgical incisions and all potential external hernia orifices were clear. She was in moderate physical condition with a mild tachycardia.
The abdominal x-rays were taken (Figure 1) which revealed dilated small bowels and no sight of gas in colon suggesting a distal jejuno-ileal obstruction. After that she was taken to CT scan. CT showed a marked dilatation of small bowels up to the terminal ileum without any sign of a mass (Figure 2). She was admitted to the ward for follow up.
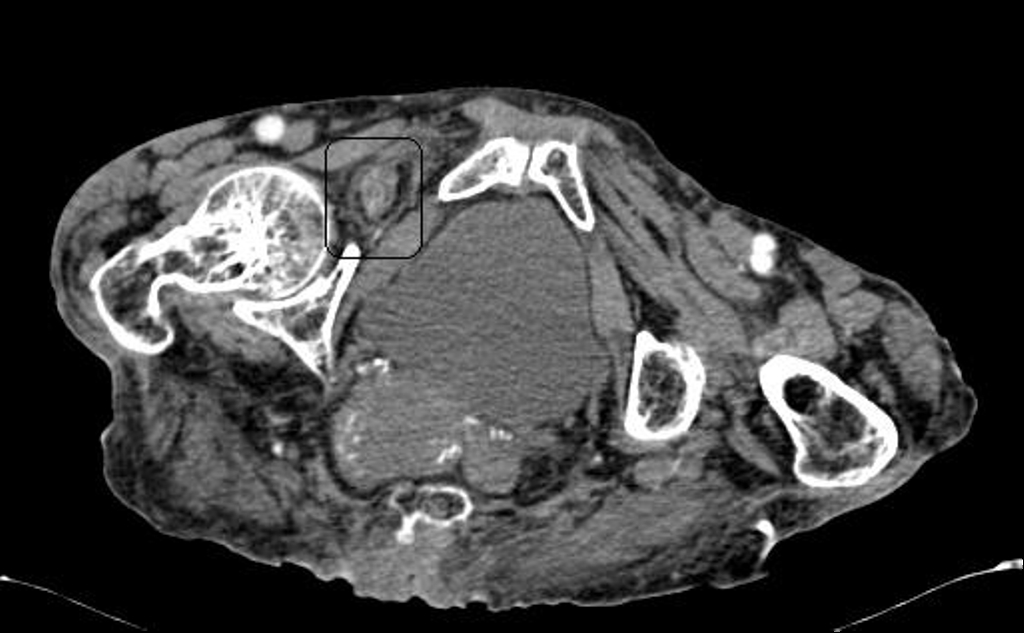
There was a cut off sign at terminal ileum just close to the right femoral canal & obturator canal at the CT scan (Figure 3).
In the ward when she was re-examined, Howship-Romberg sign was found to be positive. Because of a prolonged obstruction, multiple ER admissions and the high suspicion of the incarcerated & strangulated obturator hernia she was taken to emergency operation.
In the surgical exploration the small bowels were extremely dilated. All small bowels were taken out of the abdomen gently and followed until the obstruction site. It was seen that in the terminal ileum close to the cecum there was an incarcerated loop in the right obturator canal. Also a perforation at the side of the terminal ileum was seen. Resection of that perforated loop was done and a two layer ileum anastomosis was done.
After the operation, she was taken in the intensive care unit (İCU) because of respiratory distress. She was followed up for 7 days in ICU. Postoperative day 5 passage of stool was observed. But, she died because of respiratory insufficiency at the postoperative day 7.
Discussion
Generally the hernias that are the source of intestinal obstruction are found in the inguinal region. They are most commonly either incarserated inguinal or femoral hernias that can be generally palpated. Not so frequently patients may present with ileus problems due to the incarserated obturator hernias. These hernias, due to their anatomic location may not be detected or palpated in the physical examination of the inguinal area.
Obturator hernias accounts for 0.07?1% of all abdominal hernias and 0.2?1.6% of all cases of the mechanical obstruction of the small bowel due to hernias 1. Even if they are really rare, they have the highest mortality rate of all the abdominal wall hernias reported to be between 13% and 40% 2.
Obturator hernia is associated with some predisposing factors. It is more frequent in women especially with a wide pelvis, more triangular obturator canal opening with a great diameter. They are generally weak patients between 70 and 90 years of age. The loss of protective pre-peritoneal fat and lymphatic tissue from aging or malnutrition facilitates the formation of this type of hernias. Some co-morbid conditions (COPD, ascites malignancies etc.), chronic constipation and multiparty also predispose patients to have an obturatorial herniation 3,4.
Howship-Romberg sign refers to pain along the distribution of the obturator nerve which is caused by compression of the nerve by the hernia sac & present in 15%?50% of obturator hernia patients 5.
There is often a delay in diagnosis and delayed surgical intervention of the obturator hernia, despite the presence of a bowel obstruction. In most cases, resuscitation was first performed and medical treatment was given for the intestinal obstruction. Some surgeons have hesitated to operate because of the patients advanced age, their underlying disease, co-morbidities and their generally debilitated condition.
Signs and symptoms resulting from obturator hernias are often vague and non-specific. Because they are not so common they may always be misdiagnosed if not suspected by the surgeon. Early diagnosis of the obturator hernia which is important in preventing complications, can be made in 100% of cases with a CT of the abdomen 6.
Conclusion
A high suspicion for obturator hernia should be maintained in the elderly female emaciated patients with chronic disease presenting with recurrent episodes of sub-ileus. Early diagnosis and treatment is important in preventing major complications, morbidity and mortality. CT can be used as an early diagnostic tool in suspicion of obturator hernia.
References
- Mantoo S K, Mak K, Tan TJ. Obturator hernia: diagnosis and treatment in the modern era. SMJ. 2009;50(9):866. [PubMed: 19787172]
- De Clerq L., et al. An elderly woman with obstructed obturator hernia: a less common variety of external abdominal hernia. JBR-BTR. 2010;93:302?4.
- Rogers FA. Strangulated obturator. In: Nyhus, LM, Harkins, JN. eds. Hernia. Philadelphia: Lippincott; 1964. pp. 637?644.
- Bjork KJ, Mucha P, Cahill DR. Obturator hernia. Surg Gynecol Obstet. 1988;167:217?22.
- Yip AW, AhChong AK, Lam KH. Obturator hernia: a continuing diagnostic challenge. Surgery. 1993;113:266?9.
- Yokoyama Y, et al. Thirty-six cases of obturator hernia: does computed tomography contribute to postoperative outcome? WJS.1999; 23:214- 6, discussion 217.
|