Abstract
Primary Chylous Peritonitis is a very rare condition resembling an acute abdomen. It is basically accumulation of a chylous ascites which is a milky fluid with a high triglyceride level. Generally it is a perioperative diagnosis made in cases that were operated for an acute abdomen. Here we present a 23 years old previously healthy male patient admitted to the Emergecy Room (ER) with an acute on set of an right lower quadrant abdominal pain, leucocytosis . Imaging studies detected free fluid in Ultrasound (US) resembling Acute Appendicitis. In the operation no surgical pathology was seen other than the free milky-fluid in the abdomen and chylous peritonitis diagnosis was made. The fluid was sampled, peritoneal wash with warm saline was performed, drains were placed. He was discharged without any complications.
Keywords :
Acute abdomen
, Primary chylous peritonitis
, Emergency surgery
Turkish Abstract
Primer şilöz peritonit, akut karın ile prezente olabilen çok nadir bir durumdur. Temel olarak yüksek trigliserid içeriği olan süt kıvamında şilöz asit birikimidir. Genellikle de akut abdomen nedeni ile yapılan operasyonlar esnasında konulan bir tanıdır. Biz bu olguda, 23 yaşında daha önceleri herhangi bir hastalığı olmayan; ani başlayan sağ alt kadran ağrısı ile acil servise gelen, lökositozu saptanan bir erkek hastayı sunduk. Ultrasonografik görüntülerinde batın içinde akut apandisiti düşündüren serbest sıvı saptandı. Ameliyatta batın içinde serbest süt kıvamında şilöz peritoniti düşündüren sıvı dışında başka bir patoloji saptanmadı. Sıvı örneklendi ve batın yıkanıp dren yerleştirildi. Ameliyat sonrası komplikasyonsuz bir şekilde hasta taburcu edildi.
Turkish Keywords :
, Akut karın
, Primer şilöz peritonit
, Acil cerrahi
Introduction
Several disorders may lead to accumulation of this triglyceride rich, milky fluid (ascitis) such as; abdominal malignancies, cirrhosis, congenital diseases, postoperative or traumatic causes. Sometimes like in our case there may not be any underlying cause or a disease leading to a chylous peritonitis and named as the ?Primary Chylous Peritonitis?.
The incidence of chylous peritonitis is reported to be between 1 in 20,000 to 1 in 187,000 in the literature 1,2. Sudden leak of chylous in to the peritoneal cavity without any underlying pathology, mimicking an acute appendicitis is a very rare form of peritonitis 3.
Case Report
Our case was a 23 years old previously healthy male with out any history of a disease. He admitted to the Emergency Room (ER) after 6 hours of onset of a sudden abdominal pain. He did not have any history of a trauma, surgery or a chronic disease.
In the ER during the examination he had only a mild tachycardia, his other vital signs were normal. On abdominal examination there was a tenderness at the right lower quadrant with a voluntary defense and an abdominal rigidity. Bowel sounds were normal and he had a passage of stool in the morning. The laboratory tests, other than the white blood cell count being 11.700 k/ul (4000-9000k/ul), were normal. The chest and abdominal X-rays were non-spesific.
Patient was taken to the ultrasonography and free fluid at the right lower quadrant was seen. For the etiology and the source of the free fluid an Oral and Intravenous contrast enhanced Computerised Tomography (CT) was performed. There was also free fluid in the abdomen in CT but there were no signs of perforation or any other surgical pathology . So the patient was decided to be operated due to the clinical and physical findings of an acute abdomen.
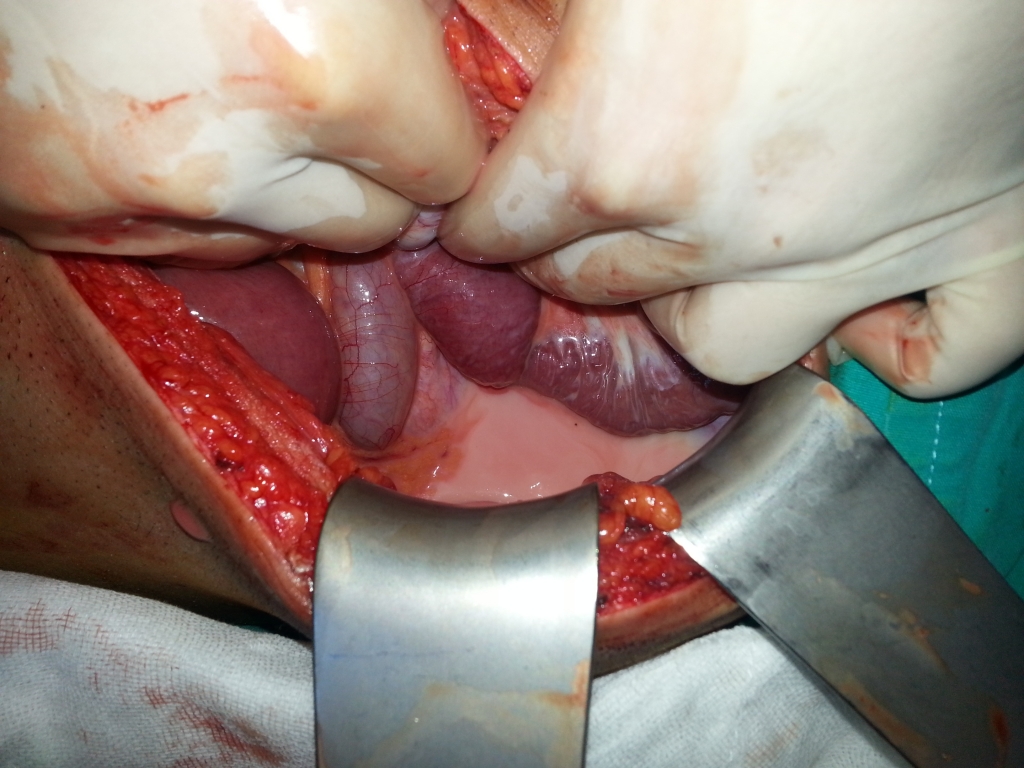
When the peritoneum was entered a milky free fluid around 200 ml came out of the abdomen. The fluid was sampled and exploration of the abdomen was done (Figure 1,2).
During the extensive abdominal and retroperitoneal exploration no cause and source of chylous was seen. After these findings the ? Primary Chylous Peritonitis? diagnosis was made.
Abdominal cavity was washed with around 5 liters of warm saline. Two large bore drains were placed into the abdominal cavity and abdomen was closed anatomically.
The peri-operative sampled fluid biochemistry results for triglyceride was reported as 1420g/dl, which was nearly ten times the normal serum triglyceride value (Normal blood value is 150g/dl).
Patient was discharged with out any complications on postop day 7. He was tested for malignancies, abdominal/thoracic masses, hematologic abnormalities etc. Nothing pathological was diagnosed.
After 6 months no recurrence of chylous ascites was seen and the patient was all normal with out any signs and symptoms.
Discussion
After the first description of this rare condition chylous peritonitis by Renner in 1910 4 there were around 100 cases reported up to today. Generally atraumatic chylous ascites is seen 85% of the times with the malignancies 5. The abdominal aortic aneurysm surgeries and retroperitoneal lymph node dissections 6 are the most common causes of surgical types of chylous peritonitis . But here in our case a much more rare condition, spontaneous chylous ascites-related peritonitis mimicking acute appendicitis is presented. İn the literature there were similar cases like ours were reported 3-7.
Generally the preoperative diagnosis can not be made in chylous peritonitis unless the percutaneous sampling of this free fluid is done preoperatively. The characteristic appereance of this milky fluid seen at the surgery helps the surgeon on making this diagnosis. The triglyceride level of this milky fluid being two to eight times that of the normal plasma triglyceride levels, which is around 150g/dl, is an important diagnosic feature of the chylous ascitis 8. In our case the triglyceride level was nearly ten times the normal plasma value (1420g/dl) .
Management of chylous peritonitis depends upon the underlying disease. In patients with symptoms of an acute abdomen, the surgical exploration must be done for the right diagnosis and the treatment. If there is a leak that can be demonstrated, than a simple surgical ligation or correction of the underlying source of the chylous leak is the choice of treatment.
In our case there were no predisposing factors like trauma or surgery and also no source was found in the surgical axploration. The extended exploration must be done in order not to misdiagnose or miss the source of this chylous fluid. There may be a retroperitoneal leak due to a trauma or secondary to a retroperitoneal dissection made before.
The suspicion of acute abdomen in surgery should be cleared from the surgeons mind by any means possible. Sometimes surgery maybe the only way to make the right diagnosis.
Laparoscopy is widely used in peritonitis cases when there is any suspicion of an intraabdominal pathology 9. But because retroperitoneal pathologies may also lead to a chylous fluid accumulation in the abdominal cavity and because securely exploring the root of the mesentery and the retroperitoneum is difficult in laparoscopic exploration, the diagnosis in almost all the cases required a laparotomy in the literature.
Conclusion
Acute Chylous peritonitis is one of the rarest acute abdomen causes that sometimes can only be diagnosed surgically. If there is no underlying cause of the free chylous seen in the surgery than the aspiration of the ascites and the lavage of the abdomen is the curative method. But the malignancy, malabsorbtion and infectious predisposing factors must be evaluated even after the surgery for any underlying disease that may lead to a chylous ascite formation. This approach was done in our case and the patient was screened, discharged and followed up until today without any problems.
References
- Almakdisi T, Massoud S, Makdisi G. Lymphomas and chylous ascites: review of the literature. Oncologist 2005;10: 632?635.
- Vasko JS,Tapper RI. The surgical significance of chylous ascites. Arch Surg 1967;95:355?368.
- Fang FC, Hsu SD, Chen CW, Chen TW. Spontaneous chylous peritonitis mimicking acute appendicitis: a case report and review of literature. World J Gastroenterol 2006; 12: 154-156.
- Renner A. Chylus als Bruchwasser beim eingeklemmten Bruch. Beitr Klin Chir 1910; 70: 695?698.
- Iwasa T, et al. Lymphangioma of the ovary accompanied by chylous ascites. J Obstet Gynaecol Res 2009; 35: 812?815.
- Combe J, Buniet JM, Douge C, Bernard Y, Camelot G. [Chylothorax and chylous ascites following surgery of an inflammatory aortic aneurysm. Case report with review of the literature]. J Mal Vasc 1992; 17: 151-156.
- Lamblin A, Mulliez E, Lemaitre L, Pattou F, Proye C. [Acute peritonitis: a rare presentation of chylous ascites]. Ann Chir 2003; 128: 49-52.
- Ward PC. Interpretation of ascitic fluid data. Postgrad Med 1982; 71: 171-13, 171-13.
- Agresta F, Ciardo LF, Mazzarolo G, Michelet I, Orsi G, Trentin G, Bedin N: Peritonitis: laparoscopic approach. World J Emerg Surg 2006; 1: 9.
|