Abstract
Thalassemias are a group of inherited anemias in which extramedullary hematopoiesis associated with ineffective erythropoiesis can be found as a complication of the disease paravertebral masses may be confronted within a broad spectrum extending from paresthesia to total paralysis. Blood transfusion, radiotherapy and surgical therapy (laminectomy, hemilaminectomy), and various medical agents can be used in its treatment.
In our case presented with back pain, we aimed to present radiological images of masses formed by the focuses of paravertebral extramedullary hematopoiesis together with the pathophysiologic development of the disease.
Keywords :
Thalassemia
, Paravertebral masses
, Extramedullary haematopoeiesis
, MRI imaging
Turkish Abstract
Talasemi inefektif eritropoeze bağlı olarak ekstramedüller hematopoez(EMH)oluşumu ile seyreden bir gurup kalıtsal kan hastalığıdır. EMH'e bağlı oluşan paravertebral kitleler ağrı , paresteziden total paraliziye kadar uzanan geniş bir klinik spektrumla karşımıza çıkabilmektedir. Tedavide kan transfüzyonu, radyoterapi ve cerrahi tedavi (laminektomi, hemilaminektomi) ve çeşitli medikal ajanlar kullanlmaktadır.
Sırt ağrısı ile başvuran olgumuzda paravertebral kitlelerin klinik yansımasını, kitlelerin radyolojik görünümlerini ,hastalığın patofizyolojik gelişimi ile birlikte sunmayı amaçladık.
Turkish Keywords :
, Talasemi
, Paravertebral kitleler
, Ekstramedüller hematopez
, MR görüntüleme
Introduction
Thalassemias are a heterogeneous group of inherited anemias characterized by defects in the synthesis of one or more of the globulin chain subunits of the adult hemoglobin tetramer hemoglobin A. In contrast to its major forms, its intermedia forms manifest themselves in later stages of life and rarely require transfusion. Over the following years, it appears as storage of iron in parenchymal tissues due to transfusion and as focuses of extramedullary hematopoiesis associated with ineffective erythropoiesis. Here, we will discuss a twenty-seven year old thalassemia patient with multiple paraspinal extramedullary hematopoiesis.
Case Report
A twenty-seven year old male patient was admitted with back pain being aggravated by movement. In addition, he had pallor and subicterus. His medical history revealed multiple blood transfusions from age two to age fourteen considering his diagnosis of heterozygous beta thalassemia. During physical examination, the palpation along the thoracolumbar vertebra trace revealed increasing sharp pain radiating to the sides bilateraly on anteflexion. His abdominal palpation revealed hepatomegaly and mild splenomegaly with patient claimed to have vague abdominal discomfort. The rest of his medical examination findings was normal.
Laboratory results revealed hemoglobin levels of 7 gr/dl, hematocrite levels of 24%, mean corpuscular volume (MCV) of 64 fL, platelet levels of 370,000 and indirect bilirubin levels of 4 mg/dl. A chest x-ray was perfomed, showing opacities, one on the right side measuring about 10 cm in diameter and extending towards the mediastinum over pulmonary hilus, the other one was on the left side being superposed with the pulmonary hilus on medial border , indistinguishable from the contour of the vertebral column (Figure 1).
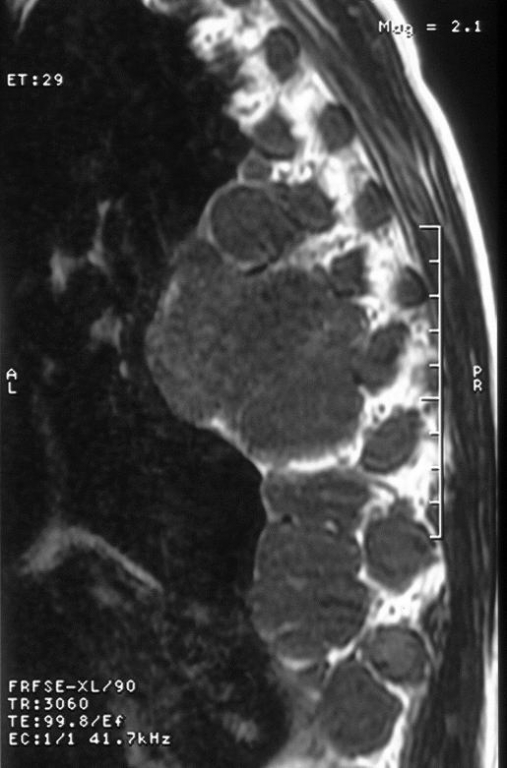
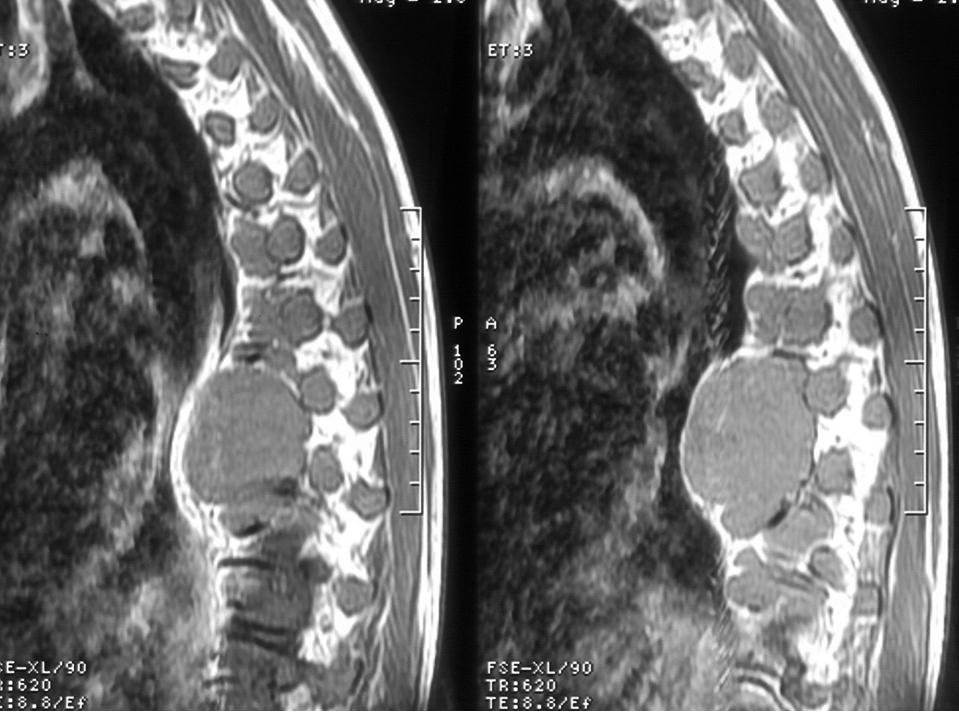
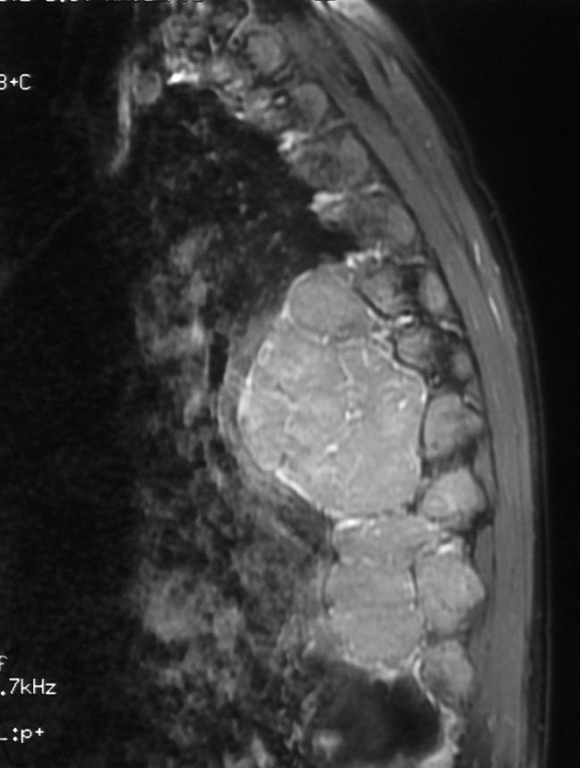
In order to diagnose these masses an MRI was performed . MRI revealed showing apparent homogenous contrasting. Paravertebral masses along the thoracic vertebra were iso-, hyperintense on T1-W and hypointense on T2-W images in comparison with the muscle signal. There were apparent homogenous contrast enhancement of masses (Figure 4a, 4b).
The masses were shown to lean on the verterbra, protruding towards neural foramina without reaching into them. Hence, the masses did not reveal any sign of neural compression nor any vertebral or costal invasion ( Fig. 5). In the light of these characteristic MRI findings and the result of the histopathological biopsy from patient?s thoracovertebral region performed one year ago, the masses were confirmed to be extramedullary hematopoiesis foci.
After the diagnosis, several blood transfusions were administered to the patient and there was a decrease in patient?s complaints. Even though the patient?s presenting symptoms were kept under control, after four weeks of treatment, there wasn?t any remission of the extramedullary hematopoiesis foci.
Discussion
Thalassemias are a heterogeneous group of inherited anemia characterized by defects in the synthesis of one or more of the globulin chain subunits of hemoglobin tetramer. Clinical syndromes in thalassemia manifest along with inadequate hemoglobin production and unbalanced accumulation of hemoglobin subunits. While inadequate hemoglobin production causes hypochromia and microcytosis, abnormal globulin accumulation causes hemolysis and ineffective erythropoiesis. According to the type of the underlying genetic defect, symptoms can be mild or very severe.
Extramedullary hematopoiesis is the production of normal blood cells out of the bone morrow. It appears as compensatory response in chronic hemolytic cases. It is encountered mostly in liver, spleen, lymph nodes, and less frequently in other tissues (kidney, adrenal glands, thymus, breast, heart, epididymis and peritoneum).
EMH in thalassemia was first described in 1954 by Gatto 1. EMH is seen in hematological diseases such as thalassemia, polistemia vera, Myleofibrozis and hemolytic anemia. It is seen less frequently in school age or adolescent period possibly due to better bone quality. Recurrent traumas and surgical interventions trigger EMH. Splenectomy increases the risk 2.
Paraspinal extramedullary hematopoiesis is seen frequently in thalassemias. Although intraspinal formation is seen in more than 11% beta thalassemias, clinical signs due to compression are rarely seen 3. No spinal cord compression was seen in a series in which 138 thalassemia patients were studied 4. Generally, it has tendency of involving middle and lower thoracic vertebrae, leading to movement restriction 5. It usually manifests as paraparesis, loss of sense and sphincter disorder. Complete paraparesis is rarely seen.
For diagnosis, MRI is the first choice, showing isointensity to spinal cord on T1-weighted (T1W) sequences, and hiperintensity on T2-weighted (T2W) sequences 6. CT myelography is the ideal diagnostic tool in detecting the localization and size of epidural masses 7. Most authors do not recommend tissue biopsy 8.
Treatment options include surgery, radiotherapy, blood transfusion and hydroxyurea. In many cases, it has been reported that when paraplegia was developed, radiation therapy was not preferred as the choice of treatment because of edema, only surgical decompression (laminectomy, hemilaminectomy) was performed. However, since hematopoietic tissues are highly sensitive to radiation, and since concurrent steroid therapy can easily prevent possible edema, radiotherapy is a proper treatment alternative 9 10--30- Gy is considered as effective dose 10. Although a nearly complete regression is seen after radiotherapy, a 19% of recurrence has been reported 6,10.
In extramedullary hematopoiesis, treating the anemia by blood transfusion leads to inhibiton of erythropoietin release and to a partial shrinkage in focuses of hematopoiesis. However, this is generally a transient improvement 11 and this is usually recommended in mild extramedullary hematopoiesis cases today 12 or may be implemented in the condition of pregnancy for the purpose of delaying surgical intervention 13.
Some authors have reported beneficial outcomes in using hydroxyurea in combination with transfusion 14. Hydroxyurea is an agent that has been used as a cytotoxic agent in myeloproliperative diseases. It has a positive effect on erythropoiesis by stimulating fetal hemoglobin production. The possibility of acute hepatoxicity and myelotoxicity development during treatment and triggering leukemic transformation in long-term restricts its use 15.
In conclusion; EMH is seen as compensatory response in patients with hemoglobinopathy. Although paraspinal masses associated with EMH are frequently encountered in thalassemias, neurologic symptoms are rare. MRI is the basic diagnostic tool. Optimal treatment approach varies according to the localization and size of the mass, and to its clinical acute status and severity.
References
- Gato I, Terrano V, Biondi L. Compressione sul spinale da proliferrazione di midillo osseonella spazio epidurale in soggetto affetto da malattia di Colley splenectomizzato. Hematologica. 1954; 38:61-75.
- Mehta J,Singhal S, Sampat NG, Mehta BC. Enlargement of paraspinal extramedullary haematopoietic mass with cord compression after splenectomy in thalassemia intermedia and response to irrradiation. J Assoc Physicians India. 1995 ;43:563-4.
- Papavasiliou CG. Tumour Simulating intrathorasic extramedullary haemotopoiesis: clinical and roentgenological considerations. Am J Roentgenol Radium Ther Nucl. 1965; 93:695-702.
- Logothetis J, et al. Thalasemia major (homozygous beta-thalassemia) A survey of 138 cases with emphasis on neurologic and muscular aspects. Neurolology. 1995; 22:294-304.
- Cook G, Sharp RA. Spinal cord compression due to extramedullary haemopoiesis in myelofibrosis. J Clin Pathol. 1994; 47:464-5.
- Munn RK, Kramer CA, Arnold SM. Spinal cord compression due to ekstramedullary hematopoiesis in beta-thalesemia intermedia. Int J Radiat oncol Biol Phs. 1998; 423:607-9.
- Khandenwal N, Malik N, Khosla VK, Suri S. Spinal cord compression due to epidural extramedullary haematopoesis in thalassemia. Pediatr Radiol. 1992; 22:70-1.
- Kaufmann T, Coleman M,Giardina P, Nisce LZ. The role of radiation therapy in the management of hematopoietic neurological complications in thalessemia. Acta Hematol. 1991; 85:156-9.
- Tan TC,Tsao j,Cheung FC. Extramedullary heamopoiesis in thalassmia intermedia presenting as paraplegia. J Clin Neurosci. 2002; 96:721-5.
- Jackson DV Jr, Randall ME, Richards F 2nd. Spinal cord compression due to ekstramedullary hematopoeiesis in thalassemia: long term follow up after radiotherapy. Surg Neurol. 1988; 29:388-92.
- Coskun E, et al. Spinal cord compression secondary to ekstramedullary hematopoeiesis in thalassemia intermedia. Eur Spine J. 1998; 7:501-4.
- Lee AC, et al. Hypertransfusion for spinal cord compression secondary to extramedullary eritropoiesis. Pediatr Hematol Oncol. 1996;13:89-94.
- Phupong V, Uerpairojkij B, Limpongsanurak S. Spinal cord compression: a rareness in pregnant Thalessemic woman. J Obstet Gyneecol Res. 2000; 262:117--20.
- Konstantopoulos K, Vagiopoulos G, Kantouni R, Lymperi S, Patriarcheas G, Georgakopoulos D, et al. A case of spinal cord compression by extramedullary eritropoiesis in thalassaemic patients: a putiative role for hydroxyurea? Hematologica 1992; 77 4:352-4.
- Najean Y, Rain JD, for the French Polycytemia Study Group.Treatment of polycytemia vera:the use of hydroxyurea and pipobroman in 292 patient under the age of 65 years. Blood. 1997 ;90:3370--77.
Information Presentation
Bu olgu 15. Ulusal İç Hastalıkları Kongresinde (2013) ve 12th European Congress of Internal Medicine (2013) de yazılı poster olarak sunulmuştur.
|