Abstract
Adnexal torsion during pregnancy is a rare event. Early diagnosis and a prompt surgical intervention are essential to prevent ovarian damage. But, the delay in diagnosis may occur due to nonspecific clinical and laboratory findings. The presented case was 9 weeks of IVF pregnancy with acute abdominal finding admitted to the Emergency Department. The Color Doppler examination of ovaries showed both venous and arterial blood flow (Class I). Transvaginal ultrasound showed an enlarged (7.0 × 7.5 cm) right ovary with heterogenous appearance and a small amount of fluid in the pouch of Douglas. The management was done conservatively. Two days later, she had again an episode of pelvic pain and no blood flow in right ovary (Class III). An emergent laparoscopy was carried out and showed a twisted right adnexa with an ischemic gangrenous ovary. The detorsion of the ovary was unsuccessful and right salpingooopherectomy was done. Postoperative period was uneventful, she delivered a healthy baby at term. This case suggested us, repeated attacks of semitorsion may endanger ovarian tissue perfusion and laparoscopic evaluation should be considered even in Class I patients with repeated attacks. In the light of this case, shortcomings in diagnosis were discussed.
Keywords :
Adnexal torsion
, Acute abdomen
, Ovarian hyperstimulation syndrome
, Laparoscopy
Turkish Abstract
Gebelik sırasında adneksiyal torsiyon nadir bir durumdur. Over hasarını önlemek için erken tanı ve hızlı cerrahi müdahele gereklidir. Fakat, tipik olmayan klinik ve laboratuvar bulguları nedeniyle tanıda gecikme olabilir. Sunulan olgu akut batın bulguları ile acil servise müracaat eden 9 haftalık in-vitro fertilizasyon (IVF) gebeliği idi. Overin renkli doppler ultrasonografi incelemesi venöz ve arteriyal akımı gösterdi (Klas I). Transvajinal ultrasonografi, büyümüş (7,0 x 7,5 cm) ve heterojen görünümlü sağ over ve Duglas boşluğundaki az miktar sıvıyı gösterdi. Tedavi konservatif olarak yapıldı. İki gün sonra, hasta pelvik ağrı ile tekrar müracaat etti ve sağ overde kan akımı izlenmedi (Klas III). Acil laparoskopi yapıldı ve torsiyone sağ adneks ile iskemik gangrenli over görüldü. Over torsiyonunun düzeltilmesi başarısız olunca sağ salpingoooferektomi yapıldı. Postoperatif dönem sorunsuz geçti ve hasta miadında sağlıklı bir bebek doğurdu. Bu olgu, tekrarlayan semitorsiyon ataklarının over doku kanlanmasını bozabileceği ve Klas I dahi olsa tekrarlayıcı atakları olan hastalara laparoskopik değerlendirme yapılması gerektiğini düşündürttü. Bu olgu ışığında tanıdaki eksik kısımlar tartışıldı.
Turkish Keywords :
, Adneksiyal torsiyon
, Akut batın
, Ovarian hiperstimülasyon sendromu
, Laparoskopi
Introduction
Adnexal torsion is defined as the rotation of the adnexa around the line of the tuboovarian ligament and the infindibulopelvic ligament that resulted in obstruction of blood flow and it is a gynecologic emergency. But, adnexal torsion in pregnancy is a rare event, with an incidence of 1-5:10.000 in spontaneous pregnancies. This incidence rises after controlled ovarian stimulation. 1 The early diagnosis is important because delay can lead to irreversible complications such as loss of the adnexa. However, delays in diagnosis and surgical intervention are relatively common due to non-specific presentation of cases and overlapping of sign-symptoms of gastrointestinal and gynecologic pathologies. 1-5
Previous studies have shown that only 23 % to 66 % of cases are given the correct presurgical diagnosis. 1,3 Although ultrasonography (US) is the primary imaging modality for evaluation of ovarian torsion, findings sometimes inconclusive. 2,4 For this reason the knowledge of clinicians about pitfalls in diagnostic procedures, gray scale and Doppler ultrasonographic evaluations before complete infarction of the ovary is important. The presented case was adnexal torsion after IVF pregnancy. The shortcomings in the diagnosis and management of pregnancies were discussed.
Case Report
A 24-year-old woman presented to the emergency department (ED) of public hospital 3 hours after the abrupt onset of right lower quadrant abdominal pain. She had 9 weeks of IVF pregnancy with controlled ovarian stimulation. She described the severe abdominal pain associated with nausea and vomiting. Similar episodes of pain and vomiting were experienced in the previous week. These were, however, shorter in duration and resolved spontaneously. There was no vaginal bleeding or bowel symptoms. The laboratory findings; complete blood count, hepatic enzymes, hematocrite and urine analysis were normal. The differential diagnosis of lower abdominal pain such as acute appendicitis, necrotic degeneration of myoma, renal colic was done via ultrasonography.
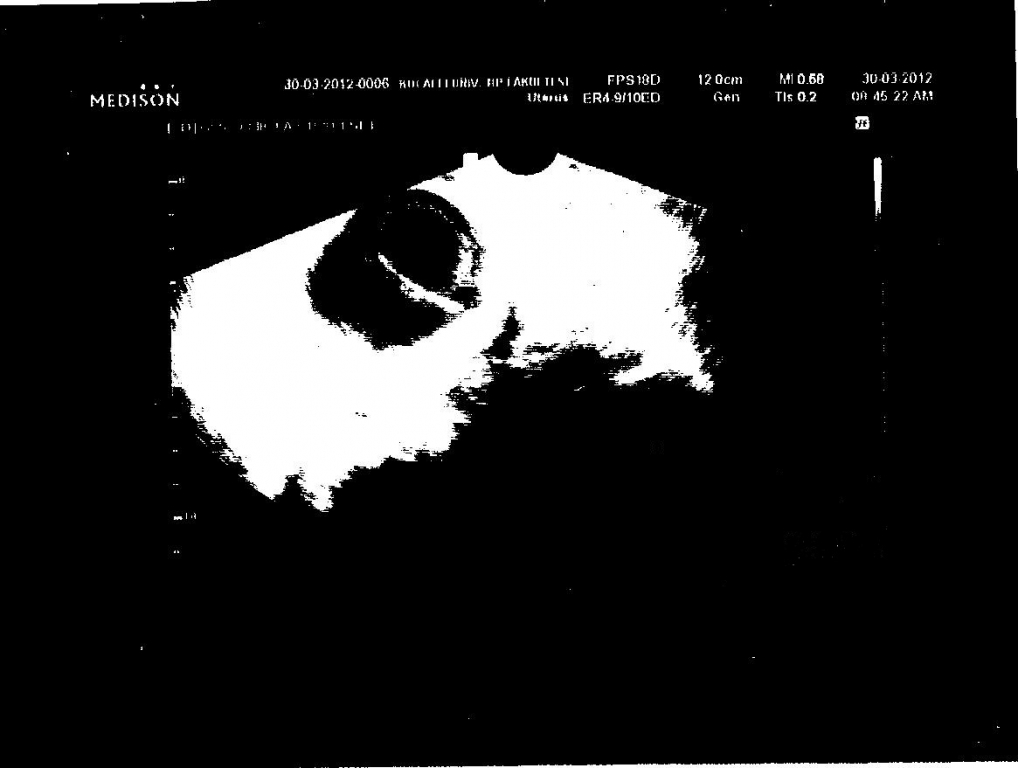
Transvaginal ultrasonographic examination showed an enlarged (7.0 × 7.5 cm) right ovary with heterogenous appearance, a small amount of fluid was revealed in the pouch of Douglas (Figure 1).
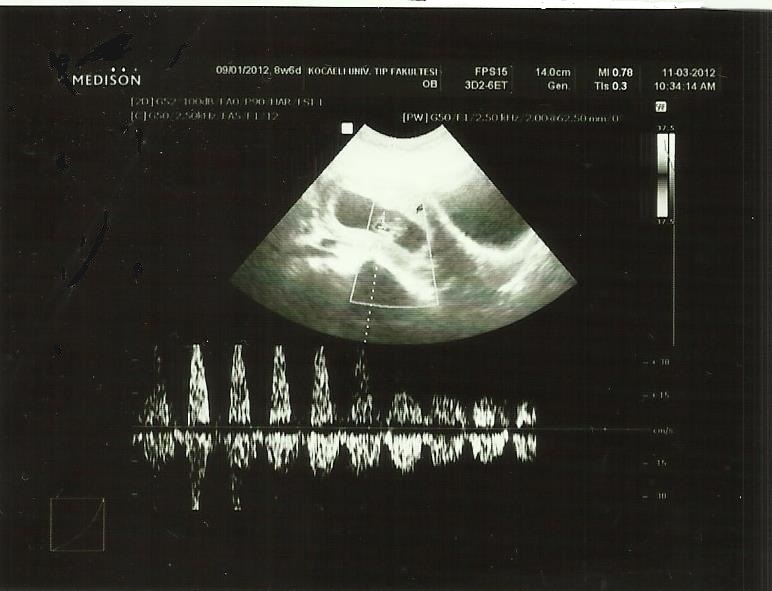
A vaginal ultrasound scan revealed a single 9- week- CRL corresponding to a fetus with regular heart rate at 170/min (Figure 2).
After that, she was referred to tertiary center with suspicion of adnexal torsion. She was hospitalized in Kocaeli University Medical Faculty, Gynecology and Obstetrics Department, with the suspicion of adnexal torsion. The Color Doppler examination showed both ovarian and intraovarian blood flow (Class I) . Her symptoms subsided and management was done conservatively. Daily gray scale and color Doppler ultrasonography was done. There were no symptoms other than hyperemesis gravidarum. Two days later, she had again an episode of pelvic pain. She underwent Doppler ultrasonography and there was no blood flow in the right ovary (Class III) . An emergency laparoscopy was done, surgical findings showed the enlarged cystic ovary was a bluish bulk large and measured about 7 cm in diameter that was three times twisted. The underwinding the twisted ovary was tried, however recoloration of adnexia was not detected. Due to gangrenous appearance of the adnexa, right salpingo-oopherectomy was performed. Surgeons did not want to run the risk of re-operation by allowing gangrenous ovary during pregnancy. The pathological findings confirmed the hemorrhagic necrosis. Postoperative period and antenal visits was uneventful, she delivered a healthy baby at term.
Discussion
Doppler ultrasonography is highly specific for the adnexal torsion, but it is not a sensitive test. 2,4 Arterial blood flow may be seen in adnexal torsion cases, leading to false-negative results. The presence of flow does not exclude the torsion, instead suggest the viability of the ovary. Since torsion may be intermittent or one of the arteries twisted (uterine or ovarian) or firstly venous thrombosis occur, blood flow may observe in Doppler findings. 2,4 The interpretation of Doppler results of adnexal torsion is variable in studies and most of them does not focus on. 6 The previous study compared the adnexal torsion cases of pregnancies with nonpregnant women, and found normal blood flow in 61 % of pregnancies and 45 % of nonpregnant women with adnexal torsion. 6
Ovarian arterial and venous blood flow are classified byAuslender. 7 This classification may be a useful guide for both diagnosis and clinical management. Class I: Both arterial and venous blood flow to the ovary is found and the conservative approach may be considered, if the clinical condition of the patient is suitable. Spontaneous resolution may take place by detorsion spontaneously. Class II: Venous flow is absent, but arterial flow preserved. This time spontaneous resolution is not seen Class III: both arterial and venous blood flow absent and ischemia exist. In patients with diagnosis of class II and III Doppler ultrasonographic findings, emergent surgical approach is needed. 7 The diagnostic and therapeutic algorithm of adnexal torsion in pregnancy was given in Table 1.
________________________________________________________________________
Table 1. The diagnostic and therapeutic algorithm of adnexal torsion in pregnancy
________________________________________________________________________
I. Gray scale ultrasonography
II. Color Doppler Ultrasonographic classification and management 7
a. Class I : Conservative management. if repeated attacks occur do laparoscopy
b. Class II : Emergenct surgical intervention
c. Class III : Emergent surgical intervention
III. If clinical suspicion persist, Magnetic Resonance Imaging (MRI) may aid diagnosis 11
__________________________________________________________________________
In our case, both arterial and venous flow were normal, the patient's symptoms subsided. Probably due to twist-untwist attacks. Sometimes as in this case incomplete torsion may occur due to uterus limit movements of ovary. However, close monitoring showed worsening of symptoms and disappearance of both arterial and venous blood flow. This case suggested us, repeated attacks of semitorsion may endanger ovarian tissue perfusion. Elective laparoscopy should be planned, if torsion-detorsion attacks occur in Class I cases. Laparoscopy may be used safely in pregnancies with suspected adnexal torsion. Todays, detorsion or detorsion and pexy in pregnant woman were recommended, owing to the advantages of laparoscopy as shorter hospital stay and favorable outcomes. Salphingo-oopherectomy is the last choice as in this case, if ischemia has already settled. 8,9,10,12
Conclusion
If pregnant women with ovarian stimulation history, present the emergency department with acute abdominal signs and symptoms, always keep in mind the risk of ovarian torsion. Loss of fertility depends on early diagnosis and prompt management. Ultrasonography is the primary imaging modality for ovarian torsion. Although the Doppler classification of ovarian torsion is useful in Class II and III cases, the presence of normal Doppler findings should not overweight clinical suspicion.
References
- Hibbard LT. Adnexal torsion. Am J Obstet Gynecol. 1985;152:456?61.
- Chang HC, Bhatt S, Dogra VS. Pearls and pitfalls in diagnosis of ovarian torsion. Radiographics. 2008; 28: 1355-68.
- Mashiach S, Bider D, Moran O, Goldenberg M, Ben-Rafael Z. Adnexal torsion of hyperstimulated ovaries in pregnancies after gonadotropin therapy. Fertil Steril.1990; 53(1): 76?80.
- Roche 0, Chavan N, Aqulina J, Rockall A. Radiological appearances of gynaecological emergencies. Insights Imaging. 2012; 3(3): 265?75.
- Krishnan S, Kaur H, Bali J, Rao K. Ovarian torsion in infertility management - Missing the diagnosis means losing the ovary: A high price to pay. J Hum Reprod Sci. 2011; 4(1): 39?42.
- Hasson J, Tsafrir Z, Azem F, Bar-On S, Almog B, Mashiach R, Seidman D, Lessing JB,Grisaru D. Comparison of adnexal torsion between pregnant and nonpregnant women. Am J Obstet Gynecol. 2010 Jun;202(6):536.
- Auslender R, et al. Doppler and gray-scale sonographic classification of adnexal torsion. Ultrasound Obstet Gynecol. 2009;34(2):208-11.
- Mathevet P, Nessah K, Dargent D, Mellier G. Laparoscopic management of adnexal masses in pregnancy: a case series. Eur J Obstet Gynecol Reprod Biol. 2003;108(2):217?22.
- Lo L-M, et al. Laparoscopy versus laparotomy for surgical intervention of ovarian torsion. J Obstet Gynaecol Res. 2008;34(6):1020?5.
- Biscette S, Yoost J, Hertweek P, Reinstine J. Laparoscopy in pregnancy and pediatric patient. Obstet Gynecol Clin North Am. 2011: 38(4),757-76.
- Lourenco AP, Swenson D, Tubbs RJ, Lazarus E. Ovarian and tubal torsion: imaging findings on US, CT, and MRI. Emerg Radiol. 2014 Apr;21(2):179-87.
- Koca YS, Yıldız I, Yılmaz E. Miad gebelikte nadir bir akut karın nedeni; Adneksiyal torsiyon. Causapedia. 2014;3:914.
|