Abstract
Mycobacterium tuberculosis today is considered an extremely rare cause of psoas abscess. It was considered the predominant cause of these abscesses in the early part of the 20th century as a result of complicated Potts disease. Extrapulmonary tuberculosis lacks specific clinical manifestation and can mimic many diseases. We report a clinical case of a 21-year-old immunocompetent male that presented with progressive right-sided back pain and weight loss due to a primary tuberculous psoas abscess. No pulmonary or spinal involvement was identified. Early diagnosis and prompt treatment with percutaneous drainage guided by ultrasound along with antituberculous drugs, lead to a satisfactory outcome.
Keywords :
Abscess
, Tuberculosis
, Psoas
, Mycobacterium tuberculosis
Turkish Abstract
Mikobakteriyum tüberkülozis günümüzde psoas apsesinin nadir bir sebebi olarak görülür. 20. yüzyılın erken dönemlerinde bu apseler Pott hastalığının bir komplikasyonu olarak görülürdü. Ekstrapulmoner tüberkülozis spesifik klinik belirtilerden yoksun olabilir ve birçok hastalığı taklit edebilir. Bu yazımızda, sağ yan-bel ağrısı ve kilo kaybı ile başvuran 21 yaşındaki hastada tüberküloza bağlı primer psoas apsesini sunduk. İmmünkompetan olan olguda pulmoner ve spinal odak saptanmadı. Erken teşhis, ultrason kılavuzluğunda perkütanöz drenaj uygulaması ve antitüberküloz ilaçlarla hasta başarılı bir şekilde tedavi edildi.
Turkish Keywords :
, Apse
, Tüberküloz
, Psoas
, Mikobakteriyum tüberkülozis
Introduction
Iliopsoas abscess (IPA) is rare, and its incidence is reported to be 0.4/100,000.It is categorized as primary or secondary, according to etiology. Primary IPA is more common in Asia and Africa, while Europe is more likely to have secondary cases 1,2.Tuberculosis is considered to be a disease of underdeveloped countries, however the incidence is rising in the western world due to increasing incidence of acquired immunodeficiency syndrome (AIDS) 3. The causes of psoas abscess have changed in the last decades. At the beginning of the 20th century, psoas abscess was believed to be mainly caused by tuberculosis (TB) of the spine (Pott's disease). However in recent years primary psoas abscess due to haematogenous spread from an occult source is more commonly encountered, particularly in immunocompromised and older patients 4,5. The most commonly affected extrapulmonary sites are lymph nodes, pleura, genitourinary tract, bones and the central nervous system, but pulmonary involvement is usually accompanied in these aforementioned sites. TB most commonly affects intestine, peritoneum, and lymph nodes in case of abdominal involvement 6,7.
In this case presentation, we aimed to report a rare primary psoas abscess due to TB infection in an immunocompetent male who has no accompanying primary focus.
Case Report
A 21-year-old Ethiopian male, who immigrated to Turkey one year before, was admitted to our emergency department in February 2014. He complained of progressive right sided-back pain during the previous 6 months and described weight loss. There was nothing abnormal in his initial evaluation except for remarkable erythrocyte sedimentation rate (ESR) elevation with a rate of 87. Anti-Human Immunodeficiency Virus (HIV) antibody tests which were repeated twice were negative. The chest roentgenogram (Figure A) and urine analysis were in normal limits.
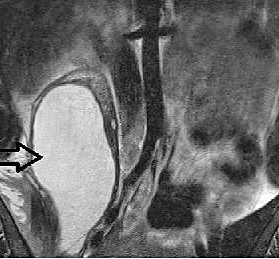
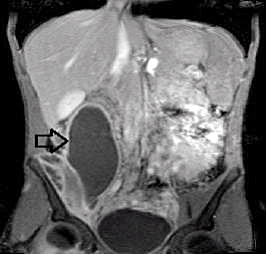
Abdominal ultrasonography showed a huge retroperitoneal cystic mass with dense content in the right abdomen involving the right psoas muscle. In order to define the borders of the lesion precisely and to reveal the extent of the disease accurately, abdominal and lumbosacral Magnetic Resonance Imaging (MRI) was performed. MRI revealed awell-defined, encapsulated cystic lesion (measuring 22.3x17.4x16.5 cm ) that enlarged right psoas muscle. Cyctic mass was hypointense on T1-weighted images, hyperintense on T2- weighted images and rim enhancement was detected after paramagnetic contrast media administration (Figure B, C).
There was no radiological evidence of spondylodiscitis (Figure D).
Due to peripheral rim-like contrast enhancement and cystic content, the diagnosis of psoas abscess was made and then the patient was referred to general surgery. After the completion of anesthesia consultations, the abscess was aspirated with ultrasound guidance in the operating room under local anesthesia. At the end of the prosedure, a 12F drainaige catheter was left in the abscess cavity. No serious complication occured during and after invasive prosedure. Seven days later when the cessation of liquid flow from drainage catheter was seen, catheter was removed. No serious complications were observed except for mild fever during hospitalization period. Abscess material was evaluated microbiologically in order to find infectious agent (s). Ziehl- Neelsen stain of the aspirate was positive for acid-fast bacilli, however cultures for bacteria or fungi were negative. Additionally, abscess culture was positive for Mycobacterium tuberculosis complex and was susceptible to all anti-TB first-line drugs. In addition to abscess drainage, anti-TB therapy was started with isoniazid (300 mg once daily), rifampin (600 mg once daily), pyrazinamide (2000 mg once daily) and ethambutol (1200 mg once daily).The patient was discharged and advised to come for follow-up monthly controls.
Discussion
The psoas abscess may be classified as primary or secondary, depending on the presence or absence of underlying disease.
The etiology of primary psoas abscess is unclear, but lymphatic and hematogenous spread of an infectious process from an occult source in the body, often associated with immunosuppressive conditions like diabetes mellitus, renal failure, intravenous drug abuse, HIV infection, malignancies and other chronic illness or trauma, has been implicated. However, in the current patient, immunosuppressive conditioncould be excluded given the medical history, negative routine blood tests, normal immunoglobulin levels and negative HIV tests.
The iliopsoas muscle lies in close proximity with sigmoid colon, appendix, jejunum, ureters, abdominal aorta, kidneys, pancreas, spine, and iliac lymph nodes. Any underlying disease in these aforementioned structures may spread to the iliopsoas muscle 3. Retroperitoneal abscesses are often polymicrobial and Escherichia coli, Klebsiella pneumoniae, Enterococcus spp., and Staphylococcus aureus are the predominant agents isolated in cultures 8.
Psoas abscess is more frequently found on the right side than the left, with rare reports of bilateral cases 9-11. The differential diagnosis of psoas abscess includes a variety of orthopedic and infectious disorders of the regional skeleton. Abdominal or retroperitoneal diseases such as renal or perinephric abscess, abdominal or pelvic abscess and regional malignancies should also be considered as the causative agents 9,12.
Psoas abscess is a diagnostic challenge in the emergency department because of it?s nonspecific symptomatology and subtle physical findings. Plain chest and abdominal radiographs may remain inadequate, on the other hand cross-sectional imaging techniques such as ultrasonography, computed tomography and MRI are useful diagnostic tools 13,14. Once the diagnosis of psoas abscess has been established, mycobacterium tuberculosis as a causative agent should firstly alert physicians thus, negligence of TB will not only delay effective therapy, but also may lead disease progression.
Therapeutic options include appropriate pharmacotherapy coupled with either surgical or radiologically guided percutaneous drainage.
References
- Shields D, Robinson P, Crowley TP. Iliopsoas abscess - a review and update on the literature. Int J Surg. 2012; 10: 466-9.
- Dietrich A, Vaccarezza H, Vaccaro CA. Iliopsoas abscess: presentation, management and outcomes. Surg Laparosc Endosc Percutan Tech. 2013; 23: 45-8.
- Kassu A, Mengistu G, Ayele B, et al. Coinfection and clinical manifestations of tuberculosis in human immunodeficiency virus-infected and -uninfected adults at a teaching hospital, northwest Ethiopia. J Microbiol Immunol Infect. 2007; 40: 116-22.
- Mallick I, Thoufeeq M, Rajendran T. Iliopsoas abscesses. Postgrad Med J. 2004; 80: 459 62.
- Berge VM, Marie S, Kuipers T, et al. Psoas abscess: report of a series and review of the literature. Neth J Med. 2005; 63: 413-6.
- Lazarus AA, Thilagar B. Abdominal tuberculosis. Dis Mon. 2007; 53: 32-8.
- Penado S, Espina B, Campo J. Absceso de psoas. Descripcion de una serie de 23 casos. Enferm Infecc Microbiol Clin. 2001; 19: 257-60.
- Brook I, Frazier EH. Aerobic and anaerobic microbiology of retroperitoneal abscesses. Clin Infect Dis. 1998; 26: 938-41.
- Dowd MD, Hegenbarth MA, Seidel FG. Case 01-1992: an 11-year-old boy with fever and a painful hip. Pediatr Emerg Care. 1992; 8: 366-9.
- Gruenwald I, Abrahamson J, Cohen O. Psoas abscess: case report and review of the literature. J Urol. 1992; 147: 1624-6.
- Vohra BK, Khanna S. Bilateral tubercular psoas abscess mimicking bilateral hydronephrosis - the role of computed tomography in the management (letter). Postgrad Med J. 1992; 68: 690.
- Goldberg B, Hedges JR, Stewart DW. Psoas abscess. J Emerg Med. 1984; 1: 533-7.
- Swartz MN. Myositis. In: Mandell GL, Doualas RG Jr. Bennett JE, eds. Principles and Practice of Infectious Diseases, 3 th New York: Churchill Livingstone Inc, 1990: 816-7.
- Sathyamoorthy P. Primary psoas abscess: case report and review of the literature. Singapore Med J. 1992; 33: 201-3.
|