Abstract
Hydatid disease is an endemic zoonosis caused by the cestode Echinococcus granulosus, and it may develop in almost any part of the body. The most common affected organs are the liver and the lungs. Echinococcal cyst located in the subcutaneous tissue constitutes an extremely rare manifestation of the hydatid disease.For this reason,especially the parts at which echinococcus granulosus is seen commonly,in spesific diagnosis of the soft tissue mass,hidatik kist should certainly be kept in mind.
Keywords :
Hydatid cysts
, Echinococcus granulosus
, Subcutaneous tissue
Turkish Abstract
Hidatik hastalık, ekinokokus granulosus sestodlarının neden olduğu endemik bir zoonozdur ve vücudun hemen her yerinde yerleşebilir. En sık etkilenen organlar ise karaciğer ve akciğerlerdir. Cilt altında ekinokok kisti,hidatik hastalığın çok nadir görülen kısmını oluşturur. Bu nedenle özellikle ekinokokus granulosusun yaygın olarak görüldüğü bölgelerde yumuşak doku kitlelerinin ayırıcı tanısında hidatik kist mutlaka akılda tutulmalıdır.
Turkish Keywords :
, Hidatik kist
, Ekinokokus granulosus
, Cilt altı doku
Introduction
Hydatid cyst disease is an endemic parasitic infestation caused by Echinococcus granulosus, and it is a health problem in the Middle East Mediterranean countries, South America, Africa, Australia and Asia.. Humans are accidental hosts and infected by oral ingestion of eggs with contaminated vegetables, water, fur or contaminated hands. Liver and lung are most often affected but hydatid disease may develop in almost any part of the body 1. Other locations are extremely rare
If parasite passes the liver and lungs, it may locate in any organ. Primary involvement of muscle and subcutaneous tissue is very rare and has been reported in approximately 3 % of all patients with hydatidosis. There are a some reports about primary subcutaneous hydatitosis in the extremities. Here we report a patient who had an isolated hydatid cyst in subcutaneous tissue, and the aim of this case report is to emphasize that patient with a mass, hydatid disease should be considered in the differential diagnosis. Furthermore, the atypical location of the hydatid cyst, as shown in the report, is a rare occasion.
Case Report
A 31-year-old female was admitted to our clinic,with a swelling of the the left gluteal region. She was seen six months after the initial occurrence of the swelling. She had no such swelling or symptoms before. Physical examination revealed a nontender diffuse, cystic swelling of approximately 8 cm in diameter, fixed to subcutaneous tissue with no evidence of local inflammation. There was no history of weight loss, trauma or fever. The diagnosis was that of a benign tumour.
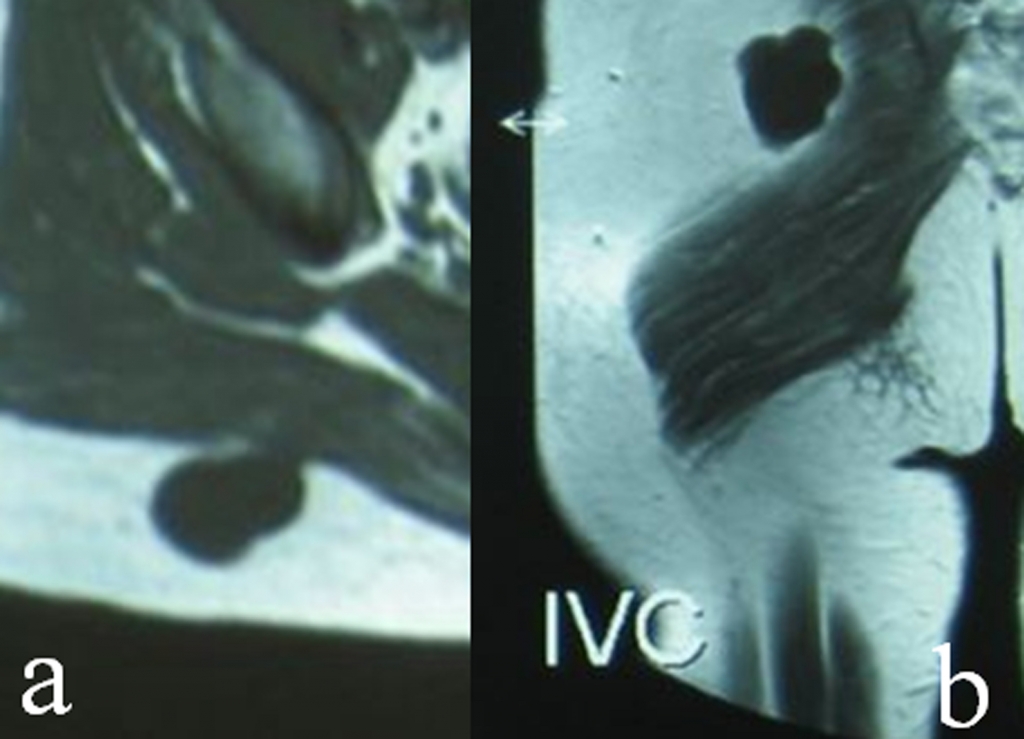
On ultrasonography, there was a cystic lesion approximately 6 × 8 cm in the subcutaneous area of the left left gluteal area. There was evidence of multiple daughter cysts within the cystic lesion, along with a few floating membranes. Probable diagnosis of subcutaneous hydatid cyst was made. There was occasional history of contact with the farm animals. X-ray of pelvis was also non contributory. Antiechinococcal IgG was positive for infection. X-ray chest and sonography of abdomen were normal. On magnetic resonance imaging a well-defined cystic lesion was seen in the left gluteal region, involving the subcutaneous fatty tissue. Preoperatively albendazole 10 mg/kg/day was given for 15 days forpresumptive diagnosis of hydatid cyst.
Fine-needle aspiration was not attempted. It is important to establish the diagnosis preoperatively in order to limit the risk of anaphylactic shock or dissemination in the event of puncture or accidental opening of the cyst during resection. During surgical exploration under general anesthesia, the skin and subcutaneous layers were incised and the cyst was reached. Hypertonic saline was injected into the cyst and after waiting for 10 min, the cyst was completely excised (Figure 2).
The cavity was irrigated with hypertonic saline and closed with a suction drain. Histologically the surgical specimen was stained with haematoxylin/eosin and confirmed the diagnosis of hydatid cyst. After operation supplementary chemotherapy with albendazole (10 mg/kg/ daily) for four months was recommended. The patient was followed for six months with no evidence of local or distant recurrence.
Discussion
The diagnosis of echinococcosis usually is based on the identi?cation of a hydatid cyst in tissue. Imaging modalities such as ultrasound and computed tomography may reveal a cyst wall and microcalci?cations within daughter cysts and varying ?uid densities between cysts and surrounding organs 2. There was no calci?cation in our case. A soft tissue hydatid cyst also can be accurately diagnosed by magnetic resonance imaging studies 3. The main factor in the diagnosis of hydatid disease in an extremity is an awareness of its possibility. Results of imaging examinations should be confirmed by serological tests, which are 80?100% sensitive and 88-96% specific for liver hydatid disease, but are less sensitive for lung and other organ involvement 4. Hydatid cysts in unusual localizations with simple cyst appearance may cause diagnostic problems..The differential diagnosis in such cases also includes chronic hematoma, and malignant soft-tissue tumors such as myxoid liposarcoma5.
It is important to establish the diagnosis preoperatively in order to limit the risk of anaphylactic shock or dissemination 6. Medical management of subcutaneous hydatidosis should be considered as adjuvant therapy to surgery. The medication should be given during the preoperative and postoperative periods with albendazole to reduce the possibility of anaphylaxis, decrease the tension in the cyst wall, and reduce the postoperative recurrence rate. Albendazole is an absorbable derivative of mebendazole, shows even greater effectiveness, because it has a higher degree of penetration into the cyst and is particularly indicated for reducing the risk of recurrence. We used it before and after the surgery.
Preoperative use of medical agents usually is impossible because early diagnosis of the disease is difficult. This problem is more prevalent in bone and spinal infestations. Hydatid cyst should be considered in the differential diagnosis of subcutaneous cysts, especially when treating patients who live in or have emigrated from areas where Echinococcus Granulosus is prevalent.
Acknowledgement
THANK YOU
References
- Doğmuş M, Kaplan M, Salman M, Yılmaz U. Unusual presence of hydatid disease in subcutaneous tissue: A case report. N England J Med. 2007;24: 246-8.
- Garcia-Diez AI, et al. MRI evaluation of soft tissue hydatid disease. Eur Radiol. 2000;10: 462-6.
- Cannon CP, et al. Soft tissue echinococcosis: a report of two cases and review of the literature. Clin Orthop Relat Res. 2001;385:186-91.
- King CH. Cestodes (tapeworms). In: Mandell GL, Bennett JE, Dolin R, editors. Principles and Practice of Infectious Diseases. ed 5. New York: Churchill Livingstone, 2000, pp 2962-3.
- Ghonge NP, Rajan S, Aggarwal B, Sahu AK. Imaging of ruptured endocyst in an isolated intramuscular hydatid cyst - The Scroll appearance. J Radiol Case Rep. Aug 2012; 6(8): 17?21.
- Tarhan NC, et al. Unusual presentation of an infected primary hydatid cyst of biceps femoris muscle. Skelet Radiol. 2002;31: 608-11.
|