Abstract
Epidermoid and dermoid cysts are benign masses and they represent less than 0.01% of all cysts of the oral cavity and neck. In this article we present two cases of large epidermoid cysts with a submental localization in an 20 and 22 year old men. Submental location was rare comparing with sublingual region. The cysts had no relationship with floor of mouth and were dissected with blunt dissection by submental neck approach. No recurrence was noticed. Epidermoid cysts are rare in head and neck region and ought to be borne in mind during the differential diagnosis of midline large neck cystic masses.
Keywords :
Submental
, Epidermoid cyst
, Large
, Neck
Turkish Abstract
Epidermoid ve dermoid kistler iyi huylu kitleler olup, oral kavite ve boyunun tüm kistlerinin %0,01 den azını temsil ederler. Bu yazıda, büyük submental yerleşimli epidermoid kistleri olan 20 ve 22 yaşlarındaki iki erkek hasta sunulmuştur. Submental yerleşim, sublingual bölgeyle karşılaştırılınca nadirdir. Hastalarımızdaki kistlerin ağız tabanı ile hiçbir ilişkisi yoktu ve kistler, submental boyun yaklaşımı ile künt diseksiyon metodu kullanılarak disseke edildi. Nüks izlenmedi. Epidermoid kistler baş boyun bölgesinde nadir görülür ve orta hatta geniş boyun kistik kitlelerin ayırıcı tanısı sırasında akılda tutulmalıdır.
Turkish Keywords :
, Submental
, Epidermoid kist
, Büyük
, Boyun
Introduction
Dermoid and epidermoid cysts are developmental benign swellings and %7 of these cysts were localized in the head and neck region 1. They represent less than 0.01% of all cysts of the oral cavity and neck 1,2.
Epidermoid cysts occur during embriyogenezis or traumatic implantation of epithelial cells into the surface epithelium 2. Histologically, they are three types as epidermoid (lined with simple squamous epithelium), dermoid (hair, hair follicles, sebaceous glands are found in the cyst wall) or teratoid ( other tissues, e.g., muscle, cartilage and bone) 3. Epidermoid cysts are observed mostly in second or third decade of life and occur more often in men than in women 2.Clinically, the lesion presents as a slow-growing asymptomatic mass, usually seen in the midline, above or below the mylohyoid muscle. If the cyst is located above the muscle, it manifests itself as a sublingual swelling, however located below the muscle, it occurs as a submental mass 4,5. Cysts may enlarged to more than one anatomical area and may reach a large size 6,7. The treatment of epidermoid cysts of the floor of the mouth and neck is surgical by two way; an intraoral or extraoral route according to the localization and the size of the mass 6,8.
In this article, we outline the two case of an epidermoid cyst with a rare giant submental component diagnosed in a 20 and 22 year old men and discuss differential diagnosis, treatment modalities and imaging techniques of these giant masses.
Case Report
Case 1
A 20-year-old man was admitted to our hospital in March 2008 with a large painless swelling at submental region of 2 years? duration. His complaint was difficulty of swallowing. His physical examination disclosed a painless, soft mass in the submental region, with no fluctuation. (Figure 1)
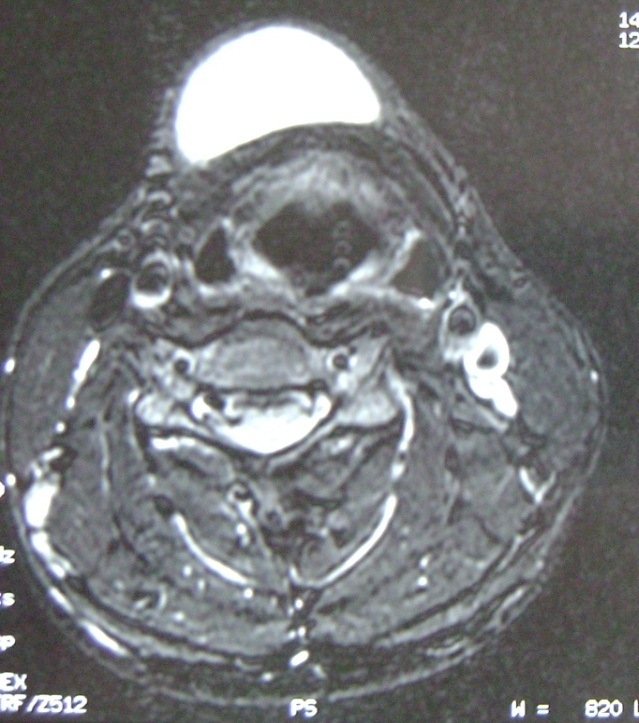
The mass did not move with swallowing or tongue motion. No adenopathies were palpated in the head and neck region. Medical history was unremarkable. A 50X50X60 mm size, soft, mobile midline mass extending from sublingual area to thyroid notch mass was found. Intraoral examination was unremarkable. An MRI scan revealed a cystic mass that filled the submental space and the mass displaced the thyrod notch posteriorly. The mass was hyperintense on T2-weighted images and hypointense on T1-weighted images without contrast enhancement. (Figure 2)
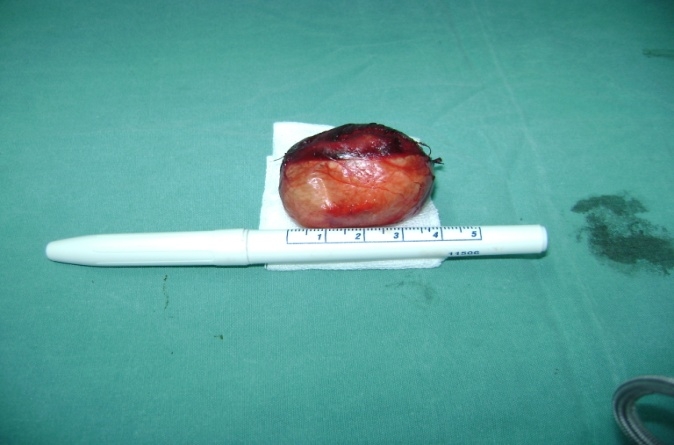
Based on these findings, surgical excision was suggested to the patient. In order to exclude thyroid pathology, thyroid scintigraphy was taken and the result was normal. Because the mass had a significant submental component (having both infra- and supramylohyoid compartments), a submental approach was preffered. A 5 cmhorizontal midline incision was made by one cm inferior to the hyoid bone. The cyst was dissected from the surrounding tissues with blunt dissection. (Figure 3,4)
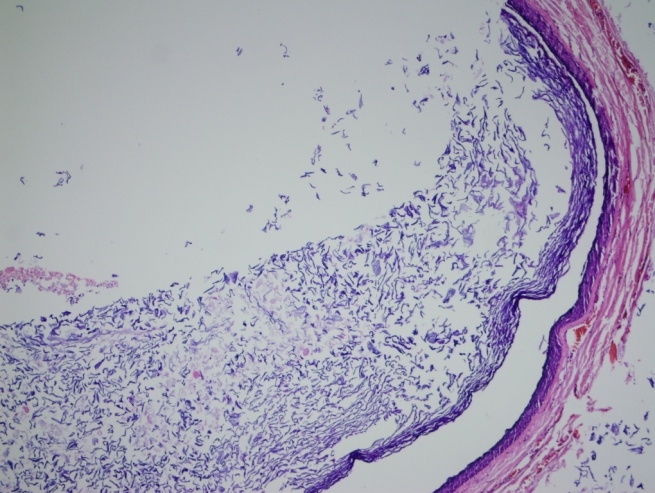
The cyst?s interior did not contain any hair or hair follicles but was filled with keratinaceous debris. Histologic sections demonstrated a cyst having a fibrovascular wall lined with squamous epithelium. The patient was followed for 12 months with no signs of recurrence.
Case 2
A 22-year-old man admitted to our hospital in September 2007 with a complaints of swelling at neck and difficulty in swallowing of solid foods for 2 years. Ear, nose and throat examination revealed 50x50x40 mm in size, a painless, soft, nonfluctuant, mobile and non-ulcerated mass at the submental region. Intraoral examination was unremarkable and any palpable lymph nodes or other masses could not palpated at head and neck region. There was no history of previous surgery or travma to oral cavity and neck. Magnetic resonance imaging of the neck revealed a lesion approximately 45X44X35 mm in size that localized at the right submental region. The mass was extending from the tiroid cartilage to the base of the hyoid bone. The MRI showed a cystic space that was hyperintense on T2-weighted images and hypointense on T1-weighted images without contrast enhancement. The mass was expanding toward the opposite submental section but not inside of the tongue or floor of the mouth. The mass caused no compression to the air column of the oropharynx and trachea. In order to exclude thyroid pathology, thyroid scintigraphy was taken and the result was normal. A5 cmhorizontal submental incision was made approximately one cm superior of the thyroid notch. The the cyst was dissected from the surrounding tissues with blunt dissection. A macroscopic view of the specimen?s ingredients revealed no mesodermal extensions, such as hair or hair follicles.(Figure 5)
Prepared histologic cross-sections revealed a cystic structure of fibrovascular walls lined with flattened and keratinaceous squamous epithelium. (Figure 6)
The patient did well postoperatively and no recurrence was noticed at the 12- months follow-up.
Discussion
Dermoid together with epidermoid cysts represent less than 0.01% of all cysts of the oral cavity 2. Our cases were at submental region and had no relationship with floor of mouth.
Many etiopathogenetical theories have been proposed. Acquired cysts derive from traumatic or iatrogenic inclusion of epithelial cells and congenital cysts o arise from ectodermic elements or may be a variant of thyroglossal duct cyst 3,5,8. Our cases had no significant history of travma and surgery so we suggested that our cases were congenital, whose their complaint was first observed at second decades. Dermoid cysts are generally diagnosed in the second and third decades of life 8; the cases presented here were an 22 and 20 years old man.
These cysts remain asymptomatic for a long time and are attached to and move with the overlying skin and may have pain when an infection occurs 3,8, rarely causing a life-threatening situation as reported by Cortezzi et al and Zachariades et al 5,9. Our cases are interfere with swelling at midline of neck and only one of the case had a swallowing problem at last for 2 years. In the differential diagnosis, : lympadenopathy, ranula, benign and malign salivary gland masses, lymphatic malformation, thyroglossal and branchial cysts and duplication foregut cyst should be in mind 6,810,11. In our cases, the hypothesis of an infection was discarded due to the period of evolution and the absence of pain and of intraoral infectious foci. Malignant tumour was ruled out in view of the lesion?s clinical aspect and the absence of lymphadenopathy.
In these cases, it is necessary to evaluate with ultrasonography, computed tomography, or magnetic resonance imaging together with cytologic examination by fine-needle aspiration biopsy 11. We do not suggest aspiration biopsy before ultrasonography, computed tomography, or magnetic resonance imaging because the borders can change and will hard to make blunt disection. Ultrasonography is the first choice for imaging, but especially for very large lesions, computed tomography and magnetic resonance imaging helps and gives more precise information for surgical approach to the cysts 7,11. An MRI scan is the preferred diagnostic tool for epidermoid cysts at our cases. They were hypointense in T1 and hyperintense in T2 MRI imaging. Our cases had no thyroid disesaes due to their thyroid scintigraphy. We suggest to do thyroid scintigraphy in order to differ thyroid disease at the diagnosis.
These cysts are named as the epidermoid cysts because they are filled with keratinaceous and lamellose material 7,8,11. In our cases, the cyst showed simple squamous epithelium without skin appendages, characterizing it as an epidermoid cyst.
In the majority of cases, epidermoid cysts are treated by enucleation 7,8,10,11 but marsupialization should be considered in cases giant cysts 7,10. Recurrence is very rare. We performed total surgical excision for both of our patients and did not observe any recurrens at follow up for one year. Mostly intraoral approach is preffered for cysts but owing to the findings for our two patients, we choosed an submental horizontal external approach because the cysts were located on the midline of the neck and not extending to floor of the mouth. Epidermoid cysts have been reported to undergo malignant transformation although this is rare 7,11.
Herein, we presented two epidermoid large cysts at submental region and this location was rare location of epidermoid cysts comparing with sublingual region and there was no relationship with floor of mouth. These cysts are benign lesions and ought to be borne in mind during the differential diagnosis of midline large neck cystic masses. Appropriate imaging techniques and thyroid scintigraphy are necessary in the preoperative diagnosis of cysts of the floor of the mouth. Surgical enucleation by submental approach is one of the effective treatment way for these large midline neck swellings.
References
- Turetschek K, Hospodka H, Steiner E. Case report: epidermoid cyst of the floor of the mouth: diagnostic imaging by sonography, computed tomography and magnetic resonance imaging. Br J Radiol. 1995; 68: 205-7.
- van der Waal I, Snow GB. Benign tumors and tumor-like lesions. In: Cummings CW, Fredrickson JM, Harker LA, Krause CJ, Richardson MA, Schuller De, editors. Otolaryngology and Head and Neck Surgery. 3rd ed. St. Louis: Mosby-Year Book, 1998; 2: p. 1407?17.
- De Ponte FS, Brunelli A, Marchetti E. Sublingual epidermoid cyst. J Craniofac Surg. 2002;13: 308-10.
- Louis PJ, Hudson C, Reddi S. Lesion of floor of the mouth. J Oral Maxillofac Surg. 2002; 60:804?7.
- Zachariades N, Skoura-Kafoussia C. A life threatening epidermoid cyst of the floor of the mouth: Report of a case. J Oral Maxillofac Surg. 1990; 48:400-3.
- Bitar MA, Kumar S. Plunging congenital epidermoid cyst of the oral cavity. Eur Arch Otorhinolaryngol. 2003; 260:223-5.
- Yilmaz I, et al. Giant sublingual epidermoid cyst: a report of two cases. J Laryngol Otol. 2006;120:19.
- Longo F, et al. Midline (dermoid) cysts of the floor of the mouth: report of 16 cases and review of surgical techniques. Plast Reconstr Surg. 2003; 112:1560-5.
- Cortezzi W, De Albuquerque E. Secondarily infected epidermoid cyst in the floor of the mouth causing a life-threatening situation: report of a case. J Oral MaxilloFac Surg. 1994;52:762?4.
- Jham B C, Duraes G V, Jham A C, Santos C R. Epidermoid cyst of the floor of the mouth: A case report. JCDA 2007; 73: 525-8.
- Kandogan T, et al. Sublingual epidermoid cyst: a case report. J Med Case Rep. 2007;1:87.
|