Abstract
We reported the third case of Brown tumor due to an atypical parathyroid adenoma.
A 65-year-old female was admitted to the hospital with a painless swelling of the right cheek and nasal obstruction. On physical examination, there was a 2×2 cm, painless mass in the right maxillary region, at the center of the alveolar part of the maxilla resulting in right nasal cavity obstruction. There was a 5x4 cm, painless, mobile mass in the right thyroid gland region and she had neither lymphadenopathy in cervical regions nor any other pathologic finding on physical examination. Brown tumor is a rare clinical condition of primary hyperparathyroidism that is most frequently caused by a parathyroid adenoma. However, the association of a brown tumor with an atypical parathyroid adenoma is extremely rare. Despite the former cases? lesions were located in the mandibula, the lesion in this case was in the maxilla.
The rarity and interesting features of brown tumors and atypical parathyroid adenomas are discussed.
Keywords :
Brown tumor
, Parathyroid adenoma.
Turkish Abstract
Literatür taramamız sonucuna göre atipik paratiroid adenomuna bağlı brown tümörünün üçüncü olgusunu bildirmekteyiz.
Altmışbeş yaşında bayan hasta sağ yanakta şişlik ve burun tıkanıklığı nedeniyle kliniğimize başvurdu. Fizik muayenede sağ maksillanın alveoler kısmının ortasında nazal kavitede obstrüksiyona neden olan yaklaşık 2x2 cm ağrısız kitle palpe edildi. Sağ tiroid gland lojunda yaklaşık 5x4 cm ağrısız mobil kitle izlendi. Servikal bölgede herhangi bir lenfadenopati ya da patolojik bulgu saptanmadı. Brown tümör sıklıkla paratiroid adenomunun neden olduğu primer hiperparatiroidizmin nadir görülen bir klinik durumdur. Bununla birlikte, atipik paratiroid adenomu ile ilişkili Brown tümörü çok nadir görülmektedir. Önceki vakaların aksine bizim olgumuzda lezyon mandibulada değil, maksillada yer almaktadır.
Bu yazımızda, atipik paratiroid adenomları ve brown tümörlerin ilginç özellikleri ve nadir görülmesi tartışılmıştır.
Turkish Keywords :
, Brown tümör
, Paratiroid adenom
Introduction
Brown tumor is a non-neoplastic lesion which develops in patients with primary or more rarely secondary hyperparathyroidism by increased osteoclastic activity and fibroblastic proliferation. The incidence of brown tumors associated with primary hyperparathyroidism is reduced because of early diagnosis of this form by routine laboratory examinations. Brown tumors are the terminal stage of bone remodeling process. Brown hemorrhagic stroma and typical giant cell formation give this tumor its name. Brown tumors of hyperparathyroidism may appear in any bone, but they are frequently found in the facial bones and jaws. Mandible is the most common site of involvement while maxillary involvement is rare 1.
We report the third case in the literature who had a recurrent brown tumor in the maxilla with primary atypical giant parathyroid adenoma.
Case Report
A 65-year-old female was admitted to the hospital with a painless swelling of the right cheek and nasal obstruction. She had first noticed the lesion 7 months ago, and it continued to increase in size and she was operated in another center. After the 3 months from the first operation, she complained about swelling in the same region of maxilla and right nasal obstruction, and was operated for the second time. Soon after this surgery, the swelling recurred for the second time and the patient was referred to our hospital.
She had a history of nephrolithiasis and hypertension. On physical examination, there was a 2×2 cm, painless mass in the right maxillary region, at the center of the alveolar part of the maxilla resulting in right nasal cavity obstruction. There was a 5x4 cm, painless, mobile mass in the right thyroid gland region and she had neither lymphadenopathy in cervical regions nor any other pathologic finding on physical examination.
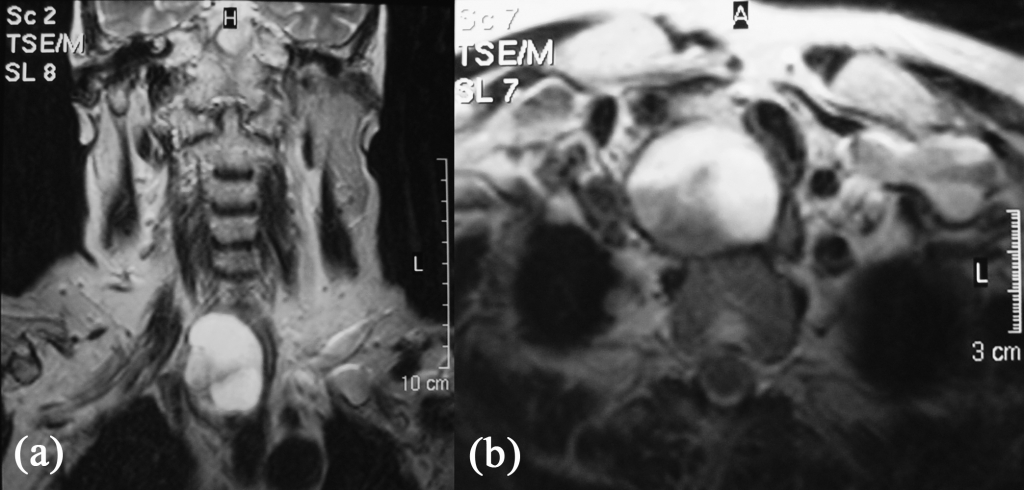
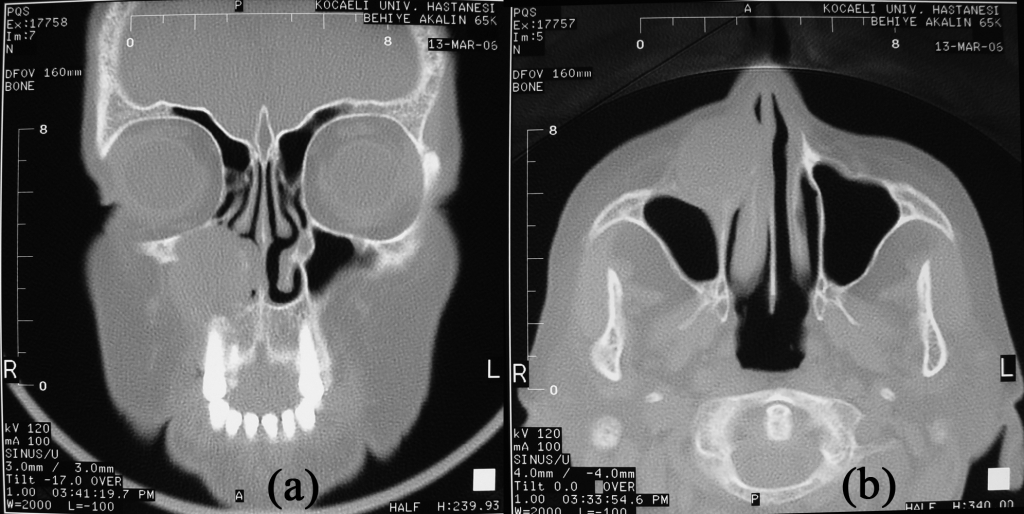
Laboratory tests revealed an elevated parathyroid hormone (PTH) level of 1109 pg/ml (normal 12?65 pg/ml) and serum calcium level of 10.9 mg/dl (normal 8.2?10.2 mg/dl) and low phosphorus level of 2.25 mg/dl (normal 2.3?4.7 mg/dl). Serum alkaline phosphatase level was 210 IU/L (N: 40?150 IU/L). Histopathologic examination of the excised maxillary mass by the second operation was reported as a central type giant cell granuloma. Plain radiographs demonstrated multiple osteolytic lesions on the pelvis and skull. Thyroid ultrasonography demonstrated a poorly demarcated, 37x41x56mm cystic nodular mass containing solid components, in the right parathyroid gland area. Magnetic resonance scans of the neck demonstrated a 5x4x3.5 cm cystic lesion that was hyperintense on T1 and T2 in the same area (Figure 1). The parathyroid scans with 15 mCi of 99mTc MIDI showed these areas as focal areas of increased activity. Computed tomography scans demonstrated a 3 cm diameter maxiller expanded lytic mass eroding the anterior wall of maxilla (Figure 2).
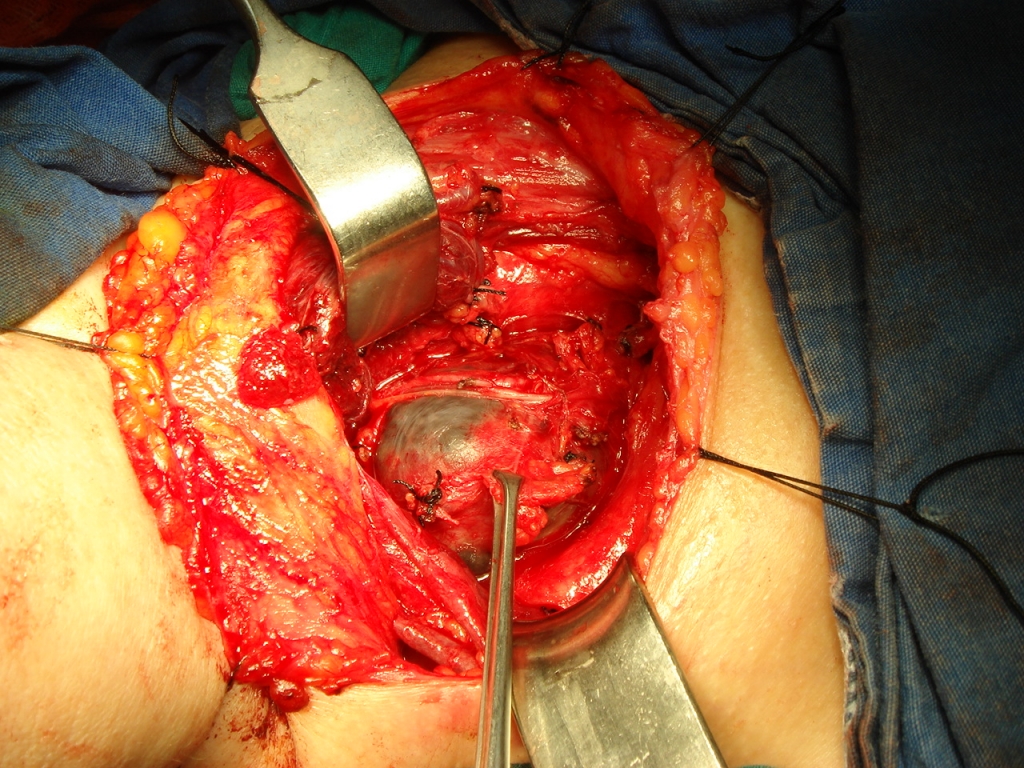
The history, physical, laboratory and radiological findings were suggestive of primary hyperparathyroidism. The patient was operated on and the right inferior parathyroid gland with adenoma was totally removed (Figure 3). The maxillary tumor giving rise to functional disability was also removed. Postoperative course was uneventful.
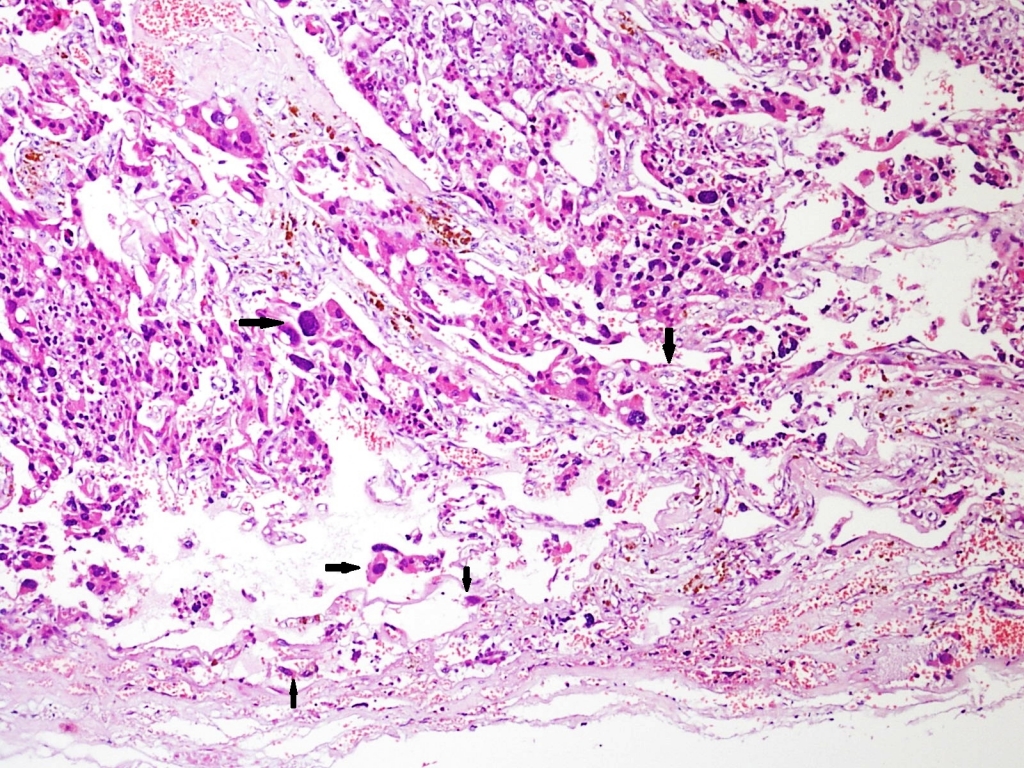
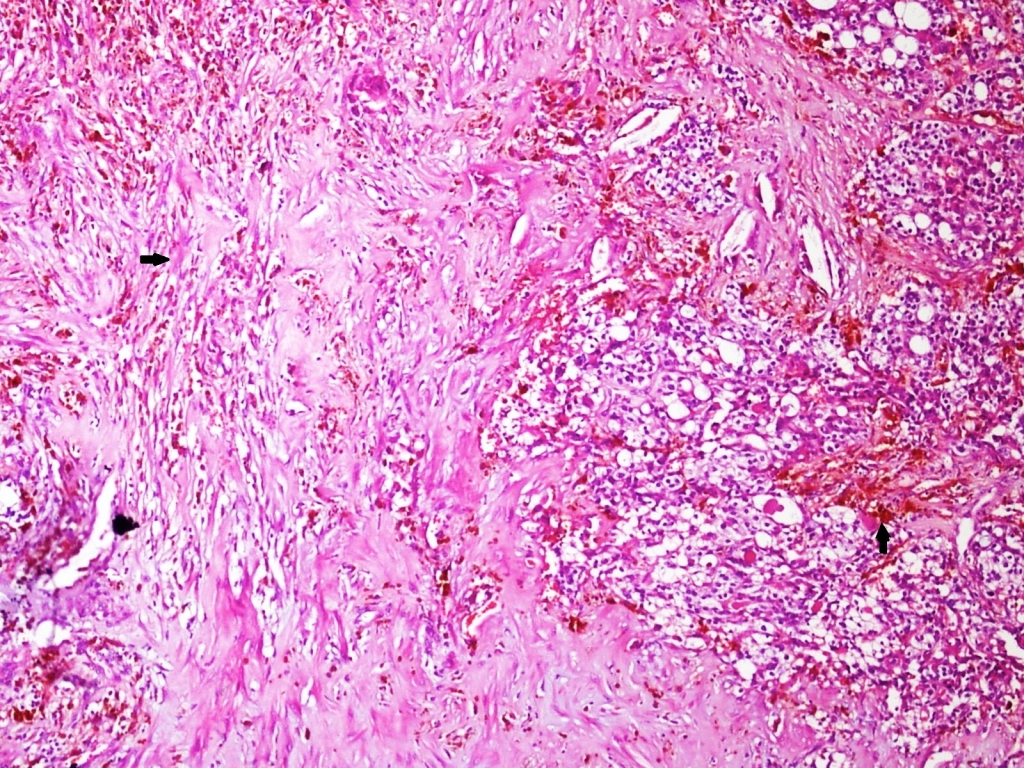
Histopathologic examination of the excised parathyroid gland revealed an atypical adenoma. The parathyroid tissue was totally encased in a fibrous capsule. Capsule varied in thickness due to entrapment of tumor cells within the capsule, but there was no obvious capsular invasion (Figure 4). Fibrous septae continuous with the capsule divided the parenchyma. Tumor cells formed wide sheets with trabecular growth pattern (Figure 5). Fibrous bands and areas of recent and old hemorrhage were noted (Figure 6). Some of the tumor cells had abundant eosinophilic cytoplasm and bizarre, hyperchromatic, highly pleomorphic nuclei without any mitotic activity and necrosis. Vascular invasion was not detected. Immunohistochemically, Ki-67 proliferation index was 1.2 %. The morphological features were consistent with an atypical parathyroid adenoma.
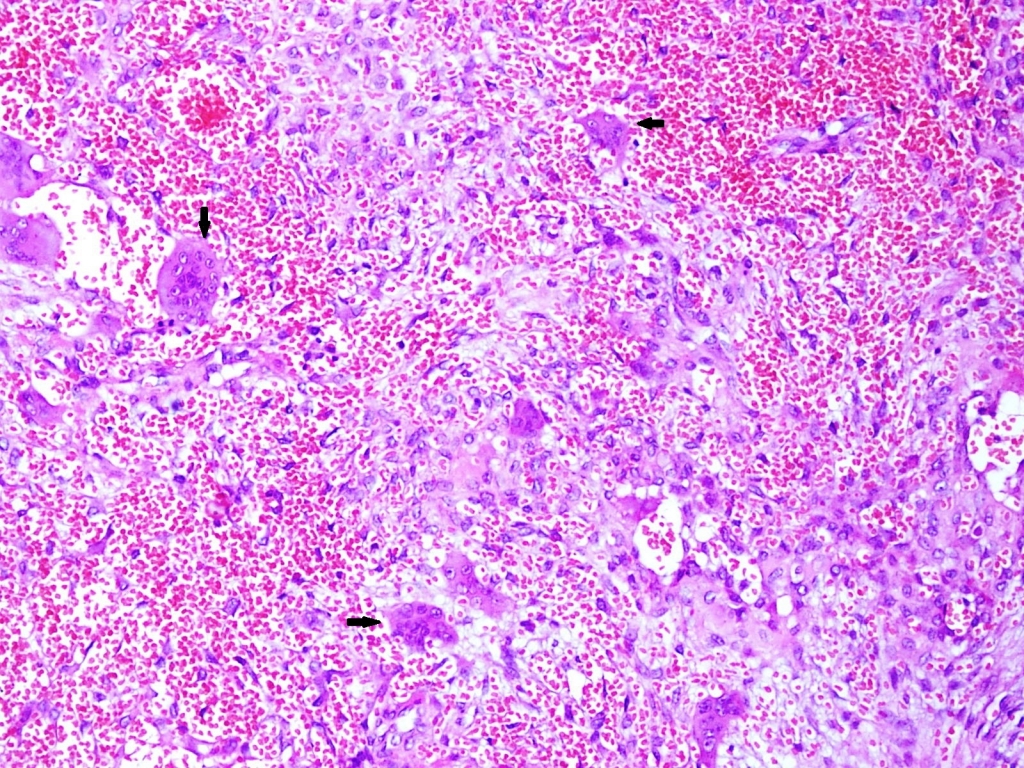
The maxillary osteolytic lesion revealed highly vascularized fibrous tissue with haphazardly scattered osteoclast-like giant cells (Figure 7). There was hemorrhage and cluster of hemosiderin laden macrophages. The histological features were typical of Brown tumor.
At follow up, two year postoperatively, the patient did not have any complaints, there were no signs of tumor recurrence, and all laboratory findings returned to normal.
Discussion
Patients with brown tumor of the maxilla usually have additional manifestations like nephrolithiasis, fatigue and weakness, nausea and bone pain, hypertension, and polydipsia and polyuria 1. In primary hyperparathyroidism, most frequent bone changes are diffuse subperiosteal bone resorption, loss of lamina dura of the teeth, and generalized osteoporosis.
Giant cell lesions of jaw like giant cell tumor, giant cell reparative granuloma, brown tumor, and cherubism are difficult to distinguish histopatologically. Therefore, clinical, radiological, and laboratory findings of hyperparathyroidism is necessary for the diagnosis and optimal therapy of brown tumors. Radiographically, disseminated brown tumors can lead to the misdiagnosis of a skeletal metastasis 2.
Osteitis fibrosa cystica (Von Recklinghausen disease) and brown tumor are not seen much as before because of early detection and treatment of hyperparathyroidism. Usually a single adenoma causes primary hyperparathyroidism, but two or more adenomas or more rarely, carcinomas can also do 3. Brown tumors are usually multiple in patients with hyperparathyroidism. Sometimes, these slowly growing and painful masses can be aggressive and destructive like a malignancy 4. These tumors can develop in any part of the skeleton, but usually are seen in the ribs, clavicle, and pelvis where the bone resorption caused by hyperparathyroidism typically occurs 1. In the head and neck region, the mandible is the most common site of involvement; however maxillary involvement like in our case is a rare condition 1.
Increased production of PTH usually causes high levels of serum total calcium and alkaline phosphatase, whereas phosphorus levels are decreased, but sometimes these levels can be normal 4. A giant atypical parathyroid adenoma can increase parathyroid hormone levels very much like a malignant tumor as in our patient. In these cases, parathyroid carcinoma can develop, so patients should go periodic follow-up with PTH and calcium levels 4.
There are several modalities for the treatment of this entity. Although some authors indicated that excising a brown tumor is not necessary when successful treatment of hyperparathyroidism is done, since the tumor tends to regress spontaneously when levels of biochemical parameters become normal 6, but increasing deformity, suspicion of malignancy or patient?s desire can be a reason for excising the tumor. Also, sometimes the tumor can grow despite the treatment of PTH metabolism 7 and enlarges after removal of parathyroid adenoma 8. Therefore, resection of brown tumor should be done if involution of the mass does not occur after the treatment of hyperparathyroidism. Surgical excision is also indicated if the lesion is large and disfiguring and or the affected bone is weakened 9. We conclude that if patients have functional deformity like ours such as nasal obstruction, surgical excision should be done, but patients with no functional problem can be followed up. Some authors use corticosteroids to reduce the size of tumor, and then excise the residual lesion 10.
Differentiation of a parathyroid adenoma from a carcinoma may be difficult, because both may share similar attributes. Capsular or vascular invasion, dense fibrous septae, mitotic figures, invasion into surrounding tissues and lymphatic or visceral metastases are common criteriae for a malignancy of the parathyroid gland 11. The signs of distant metastasis or local invasion findings are important for pathologists when making diagnosis of parathyroid carcinoma by microscopic examination 12.
The term ?atypical adenoma? has been used to refer to parathyroid neoplasms without signs of capsular or vascular invasion but exhibiting several features similar to those of parathyroid carcinoma. These features include broad fibrous bands with or without hemosiderin deposits, mitoses, and neoplastic cell groups in a thickened fibrous capsule and trabecular growth pattern 1,3.
Atypical adenomas are tumors of uncertain malignant potential. The clinical behavior of this tumor is unpredictable. Levin et al. reported ploidy results and follow-up in 12 cases of atypical adenomas 4. The 2 patients with aneuploid pattern developed recurrent disease while the remaining 10 patients with non-euploid pattern did not have any evidence of disease with an average follow-up of 2 years. Stojadinovic et al. reported no evidence of recurrent or metastatic disease in 8 cases of atypical adenomas; however their follow-up was limited.3 The atypical adenoma case presented by mandibular Brown tumor reported by Suarez-Cunqueiro et al. did not have any evidence of disease in 3 years 1.
There are two brown tumors with atypical parathyroid adenoma reported in the English literature. These tumors were seen in the mandibula. This is the first time a brown tumor with atypical adenoma has been seen in the maxilla on contrary to the former cases.
Conclusion
Patients with central giant cell containing lesions should be screened for hyperparathyroidism and hypercalcemia. Histologically, Brown tumor, giant cell granuloma, giant cell tumor, cherubism, and aneurysmal bone cyst have similar, if not indistinguishable, features. Definitive diagnosis relies on detailed analysis of clinical, radiological and biochemical findings. Atypical parathyroid adenomas have uncertain malignant potential; therefore, these patients should follow up closely.
References
- Merz MN, Massich DD, Marsh W, Schuller DE. Hyperparathyroidism presenting as brown tumor of the maxilla. Am J Otolaryngol. 2002;23:173-6.
- Gupta A, Horattas MC, Moattari AR, Shorten. SD. Disseminated Brown tumors from hyperparathyroidism masquerading as metastatic cancer: A complication of parathyroid carcinoma. Am Surg. 2001;67:951-5.
- Goshen O, Aviel-Ronen S, Dori S, Talmi YP. Brown tumour of hyperparathyroidism in the mandible associated with atypical parathyroid adenoma. J Laryngol Otol. 2000;114:302-4.
- Suarez-Cunqueiro MM et al. Brown tumor of the mandible as first manifestation of atypical parathyroid adenoma. J Oral Maxillofac Surg. 2004;62:1024-8.
- Silverman S Jr., Ware WH, Gillooly C Jr. Dental aspects of hyperparathyroidism. Oral Surg Oral Med Pathol. 1968; 26:184-9.
- Akinosi HO, Olumide F, Ogunbiyi TA. Retrosternal parathyroid adenomas manifesting in the form of a giant-cell ?tumor? of the mandible. Oral Surg Oral Med Pathol. 1975; 39:724-34.
- Dusunsel R, et al. Maxillary brown tumor caused by secondary hyperparathyroidism in a boy. Pediatr Nephrol. 2000;14:529-31.
- Yamazaki H, Ota Y, Aoki T, Karakida K. Brown tumor of the maxilla and mandible: Progressive mandibular brown tumor after removal of parathyroid adenoma. J Oral Maxillofac Surg. 2003;61:719-22.
- Pellegrino SV. Primary hyperparathyroidism exacerbated by pregnancy. J Oral Surg. 1977;35:915-7.
- Martinez-Gavidia E.M, et al. Highly aggressive brown tumour of the maxilla as first manifestation of primary hyperparathyroidism. Int J Oral Maxillofac Surg 2000;29:447.
- Vasquez-Quintana E. Parathyroid carcinoma: Diagnosis and management. Am Surg 1977;63:954-957.
- Sandelin K. Parathyroid carcinoma. Cancer Treat Res 1997;89:183-192.
|