Abstract
There are numerous causes for chronic cheek swelling, including masseteric hypertrophy, lymphadenopathy, diffuse inflammatory changes and neoplasia. Adenoid cystic carcinoma of the accessory parotid gland is extremely rare. We present a case of a 42-year-old female with adenoid cystic carcinoma arising in the accessory parotid gland. She had complained of a painless and round mass of the right cheek for a duration of 3 years. Ultrasonography, fine-needle aspiration cytology and MRI were performed preoperatively. The tumor was removed without facial nerve injury via a midcheek skin incision. We didn't add radiotherapy to our treatment. A close follow-up is planned and applied.
Keywords :
Accessory parotid gland
, Adenoid cystic carcinoma
Turkish Abstract
Yanakta uzun süren şişkinliğin, masseter kas hipertrofisi, lenfadenopati, yaygın inflamatuar değişiklikler ve neoplazi gibi çok sayıda nedeni vardır. Aksesuar parotis glandında, adenoid kistik karsinom son derece nadir izlenir. Bu makalede, aksesuar parotis glandından kaynaklanan adenoid kistik karsinomu olan 42 yaşında bir kadın hasta sunuldu. Hastanın üç yıldır yanakta ağrısız kitle şikayeti mevcuttu. Hastaya, ameliyat öncesi ince iğne aspirasyon sitolojisi, ultrasonografi ve magnetik rezonans (MR) görüntüleme yapıldı. Tümör, fasiyal sinir hasarı olmadan orta yanak insizyonu ile çıkartıldı. Hasta yakın takibe alındı.
Turkish Keywords :
, Aksesuar parotis glandı
, Adenoid kistik karsinom
Introduction
The differential diagnosis of masses in the mid-anterior cheek area includes lesions arising from normal anatomic structures as well as from variations like accessory parotid gland tissue. The accessory parotid gland is a small unit of salivary gland tissue lying on the masseter muscle craniolateral to the Stensen?s duct but separated from the main portion of the parotid gland 1. The reported incidence of accessory parotid glands observed by autopsy studies ranges from 21% to 56% 1,2. The histology, variety, and distribution of accessory parotid gland neoplasms are similar to neoplastic processes of the main parotid gland but occur much less frequently, because of the rarity of this anatomical variation 1,3. These tumors usually present as midcheek swelling, and surgical approaches are controversial. The incidence of the tumors arising in the accessory parotid gland ranges from 1 to 7.7% of all parotid gland tumors 3,4. Johnson and Spiro ,5 reported that more than half of accessory parotid gland tumors were malignant.
Adenoid cystic carcinoma (ACC) was first described by Billroth in 1856 and called cylindroma. ACC is a rare tumour entity and forms about 1% of all malignant tumours of the oral and maxillofacial region and about 22% of all malignant tumours of the major and minor salivary glands ,6. In the present report, we describe a case of adenoid cystic carcinoma arising from accessory parotid gland, and to our knowledge, there is only one case reported before 5.
Case Report
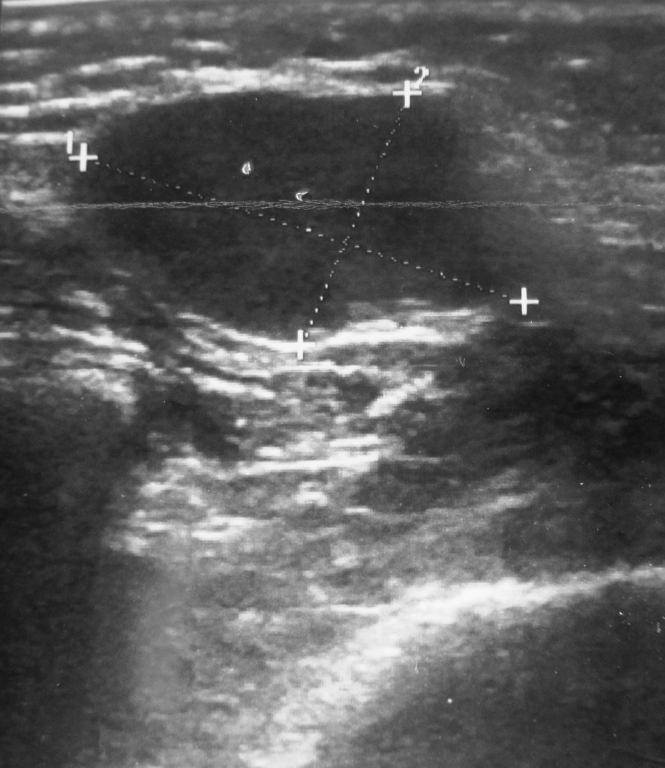
A 42-year-old woman was referred to our university hospital because of a painless, asymptomatic, slow-growing mass of the right mid-anterior cheek of 3 years duration. Physical examination revealed a 2 x 1.5 cm rubbery hard mass which was freely movable. The tumor did not adhere to the skin. There was no remarkable abnormality in her oral and nasal cavities. No lymph node swelling was observed in her head and neck. The patient exhibited no neurological deficits. Laboratory data were within normal limits. An ultrasonography showed a 19x11mm well-defined hypoechoic mass on the masseter muscle (Figure 1).
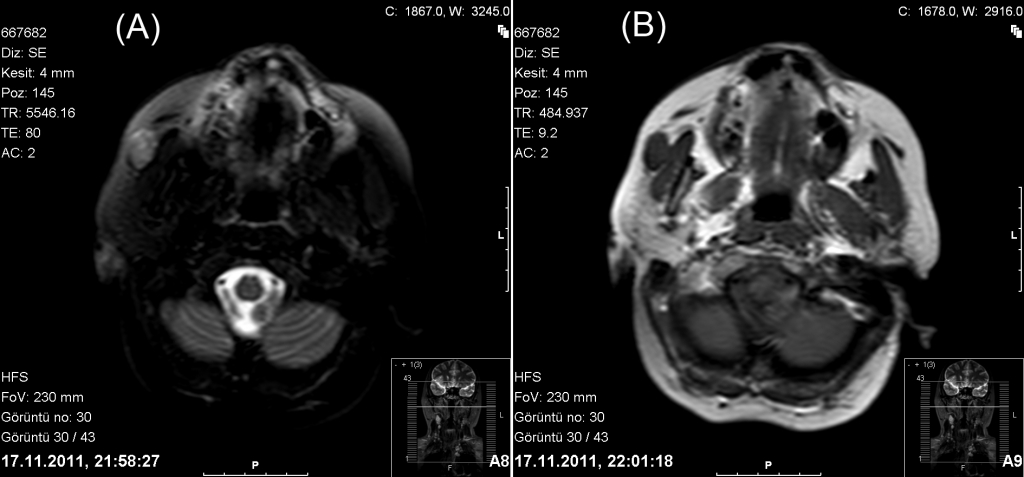
Magnetic resonance imaging revealed a tumor 18 mm × 20 mm in diameter located anterior to the right masseter muscle, which showed high intensity on the T2 weighted images and on gadolinium-enhanced T1-weighted images, the high-intensity area was seen in peripherally (Figure 2).
These findings suggested it to be a tumor arising in the accessory parotid gland. Result of cytologic examination after fine-needle aspiration cytology suggested that this tumor was an adenoid cystic carcinoma. A midcheek skin incision was made under general anesthesia and a dissection was performed (Figure 3).
The buccal branch of the facial nerve and Stensen?s duct were identified . Adhesion between the nerve branches and the tumor was not seen. The tumor and the remaining accessory gland were removed with intratumoral part of the main duct. The Stensen ducts were anastomosed and a thin catheter was used to keep the duct open followed by suturing the defect; then the catheter was removed through the mouth 7 days after surgery. The final result of the cytologic examination revealed that this tumor was a tubular pattern of the adenoid cystic carcinoma of the right accessory parotid gland. After surgery, neither facial nerve palsy, nor salivary fistula were found and recurrence has not been seen to the present.
Discussion
Accessory parotid gland tumor is often noticed as a painless and firm mass in the mid-portion of the cheek. Various differential diagnoses must be considered in patients presenting with a mass in the mid-anterior cheek. These include inclusion cysts, lymphadenopathy, hemangiomas or arteriovenous malformations of the anterior parotid gland, lipomas, neurofibromas, schwannomas, neurilemmomas, fibromas, metastasis of malignancies, and sialocoeles. Intramasseteric hemangioma, tumours of the anterior extension of the main parotid gland, sialolithiasis, and heterotopic salivary tumors. Accessory parotid gland lesions should also be considered in the differential diagnosis. It is sometimes hard to reach the final diagnosis clinically. The physical examination always reveals a solid mass in the midcheek, and the mass is always palpable, moderate to hard in hardness, without tenderness, mobile, and with clear boundary. For preoperative diagnosis, ultrasonography, MRI and fine-needle aspiration biopsy were performed in our case and they were useful for a diagnosis by detecting the size, shape, histology and location of the tumor. MRI was useful for determining the surgical approach to the mass, clarifying relationships between the mass and adjacent structures such as the Stensen duct and the masseter muscle. Fine-needle aspiration biopsy is usually useful for the preoperative histologic diagnosis of tumors in the head and neck regions.
The tumor of the present case was grossly separated from the parotid gland. As the tumor was located on the masseter muscle and a histologically normal salivary gland was observed in the periphery of the tumor. The most common tumor arising in the accessory parotid gland is benign pleomorphic adenoma, followed by mucoepidermoid carcinoma 3,5. The main symptom in the majority of these cases was acute, chronic or intermittent cheek swelling. It is estimated that 35?50% of accessory parotid gland tumours are malignant, which is more than the 25% malignancy rate reported for the parotid gland 1. Adenoid cystic carcinoma originating in the accessory parotid gland are extremely rare. To our knowledge, this is the second case of a adenoid cystic carcinoma emerging from the accessory parotid gland 5. Generally, adenoid cystic carcinoma occurs in most cases in the fifth or sixth decade of life and is slightly more common in women than in men 7. Our patient was female too. Surgery was the prime treatment and the neck dissection was performed in the presence of clinically or radiographically positive lymphadenopathy. We did not perform a neck dissection because there were no palpable or radiologic lymphadenopathy. The disease is characterized by slow progression and late onset of distant metastases, leading to treatment failure. Up to date, the optimal treatment strategy of ACC remains unclear. Negative prognostic factors identified in previous studies include increasing stage of tumor, presence of cervical metastases, predominantly solid histological features, positive margins of resection and perineural invasion. These factors have been suggested as the indication for postoperative radiotherapy in ACC. We haven't encountered any negative prognostic factors in the present case, the surgical margins were clear of tumor and no perineural invasion is seen in pathological examination. Recently, numerous studies have shown a benefit in local-regional control and long survival for ACC patients when surgery and radiotherapy are combined, especially for those with unfavorable prognosticators such as advanced lesions 8,9. However, even with the combined modalities, the results have remained suboptimal and many patients experience local failures in long run. Therefore, some authors postulate that postoperative radiation likely delays rather than prevents recurrences 10. In this case, we did not add radiotherapy to our treatment. There were no negative prognosticators. A close follow-up is planned and applied.
Surgical approaches to tumors arising from the accessory parotid gland include a midcheek skin incision overlying the tumor, an intraoral approach, a parotidectomy-type incision without a parotidectomy, a standard parotidectomy, and a face-lift approach 5,11. Rodino recommends that the best surgical approach to tumours in the accessory parotid region is via a standard parotid incision and concomitant superficial parotidectomy 12. The parotidectomy approach is not free of disadvantages or risks 5. The wide dissection can lead to surgical trauma to the facial nerve and to the risk of an iatrogenic lesion, morbidity is higher, complete recovery takes longer than with direct access, and operating and hospitalization times and costs are increased. Perzik and White commented that to manage every tumor with a formal superficial parotidectomy and full facial nerve dissection would increase morbidity with little added benefit 3. Being located anterior to the masseter muscle, a removal of the accessory parotid gland transorally, with the nerve monitor applied and the Stenson?s duct cannulated might be an appropriate approach as well. Nevertheless, an intraoral approach provides inadequate exposure for control of bleeding and for preservation of the facial nerve. Intraoral access and skin incisions have some interesting advantages. These approaches are easier and quicker to perform than parotidectomy accesses, and the intraoral approach does not cause any esthetic problem, similarly to skin incisions when performed in skin creases 13. Our patient's radiological and physical examination findings are directed us to an external operation. We thought that although an intraoral approach has a very good cosmetics, it probably will not be enough to control the tumour's margins adequately. We performed a mid-cheek incision was performed, and no facial nerve damage was observed postoperatively. With the chosen external approach, we caused a scar in our patient's face, but it ensured to us a good exploration of the facial nerve branches, Stensen duct, and entire margins of the tumour. During the surgical process, the buccal branches of the facial nerve were identified and preserved carefully, the Stensen duct was partially resected, and re-anastomosed. In addition, a thin catheter was used to keep the duct open followed by suturing the defect; then the catheter was removed through the mouth 7 days after surgery.
For the accessory parotid malignancies, surgical resection plus postoperative radiotherapy has been most used and has produced good results for mucoepidermoid carcinoma, squamous cell carcinoma, carcinoma ex pleomorphic adenoma, basal cell adenocarcinoma, and undifferentiated carcinoma 14. On the other hand, Kokemueller reported the difference between local control rates of patients with postoperative radiation and patients without postoperative radiation did not show any significance 15. Further prospective studies should be performed to clarify the benefit of postoperative radiotherapy in accessory parotid malignancies. In the present study, we performed only surgery and will follow the course of the patient.
We have no prognostic data on the adenoid cystic carcinoma of the accessory parotid gland because of its rarity. Therefore, careful and periodical follow-up is being continued. Further additional reports will provide more details on this condition and so, more accurate estimations on prognosis and more right preferences on treatment modalities can be achieved.
References
- Frommer J. The human accessory parotid gland: its incidence, nature, and significance. Oral Surg Oral Med Oral Pathol. 1977;43:671?6.
- Toh H, et al. Incidence and histology of human accessory parotid glands. Anat Rec. 1993;236:586?90.
- Perzik SL, White IL. Surgical management of preauricular tumors of the accessory parotid apparatus. Am J Surg. 1966;112:498?503.
- Polayes IM, Rankow RM. Cysts, masses and tumors of the accessory parotid gland. Plast Reconstr Surg. 1978;64:17?23.
- Johnson FE, Spiro RH. Tumors arising in accessory parotid tissue. Am J Surg. 1979;138:576-8.
- Brown JS. Prognostic factors in oral, oropharyngeal and salivary gland cancer. In: Booth PW, Schendel SA, Hausamen JE, ed. Maxillofacial Surgery (Volume 1). Edinburgh London New York: Churchill Livingstone, 1999: 291?308.
- World Health Organization. Classification of Tumours. Pathology and Genetics of Head and Neck Tumors. Lyon: IARC Press, 2005.
- Garden AS, et al. The influence of positive margins and nerve invasion in adenoid cystic carcinoma of the head and neck treated with surgery and radiation. Int J Radiat Oncol Biol Phys. 1995;32:619?26.
- Chen AM, et al. Adenoid cystic carcinoma of the head and neck treated by surgery with or without postoperative radiation therapy: prognostic features of recurrence. Int J Radiat Oncol Biol Phys. 2006;66:152?9.
- Spiro RH. Distant metastasis in adenoid cystic carcinoma of salivary origin. Am J Surg. 1997;174:195?8.
- Chang CH, et al. Cavernous vascular tumor of the accessory parotid gland. J Craniofac Surg. 2007;18:1493-6.
- Rodino W, Shaha AR. Surgical management of accessory parotid tumors. J Surg Oncol. 1993;54:153?6.
- Lewkowicz A, et al. Accessory parotid gland masses. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89:610-2.
- Sun G, et al. Diagnosis and treatment of accessory parotid-gland tumors. J Oral Maxillofac Surg. 2009;67:1520-3.
- Kokemueller H, et al. Adenoid cystic carcinoma of the head and neck, a 20 years experience. Int J Oral Maxillofac Surg. 2004;33:25?31.
Information Presentation
34th Turkish National Congress of Otorhinolaryngology and Head and Neck Surgery, October 10-14, 2012, Antalya, Turkey.
|