Abstract
Angina or acute coronary syndrome triggered by coronary vasospasm with allergic reaction, is called Kounis syndrome.Although Kounis syndrome is a well-known entity in cardiology practice, many patients still cannot be diagnosed for various reasons. A 38-year-old male patient was admitted to the emergency department with dyspnea, nausea, and chest pain. On the electrocardiogram, there was ST segment elevation at precardial derivations, especially at V2 and V3 derivations.An immediate coronary angiography was performed with the diagnosis of anterior miyocardial infarction.Normal coronary anatomy was detected. From the detailed anamnesis, it was learned that the patient was a heavy smoker and was using amoxicillin trihydrate 1000 mg, paracetamol 250 mg, oxolamine citrate 100 mg, and clorpheniramine maleate 2 mg orally and terbutaline sulphate as an inhaler for flu and cough. With these signs and symptoms the diagnosis was thought to be Kounis syndrome induced by amoxcillin. The lack of typical anaphylactic signs and symptoms were thought to be because of the oral antihystaminic and inhaler betamimetic drugs he used at the same time. A detailed anamnesis of acute coronary syndrome will provide correct diagnosis, treatment, and follow for of patients and prevent unnecessary interventional procedures.
Keywords :
Kounis syndrome
, Atypical
, Amoxicillin
Turkish Abstract
Allerjik semptomlar ile birlikte koroner vasospazm sonucu ortaya çıkan angina ve akut koroner sendrom Kounis sendromu olarak adlandırılmaktadır. Kounis sendromu kardiyoloji pratiğinde iyi bilinmesine rağmen pek çok hasta çeşitli nedenlerle hala tanı alamamaktadır.
Otuz sekiz yaşında erkek hasta acil servise göğüs ağrısı, nefes darlığı ve bulantı şikayetleri ile başvurdu. Elektrokardiyografide V2 ve V3 derivasyonlarında daha belirgin olmak üzere tüm prekordiyal derivasyonlarda ST segment elevasyonu izlendi. Hastaya akut anterior miyokard enfarktüsü ön tanısı ile acil koroner anjiyografi yapıldı. Ancak normal koroner anatomi saptandı. Hastanın medikal öyküsü sorgulandığında yoğun sigara içicisi olduğu, soğuk algınlığı ve öksürük şikayetleri nedeniyle amoksisilin trihidrat 1000 mg, 250 mg parasetamol, 100 mg oksolamin sitrat, 2mg klorfeniramin maleat oral, inhaler olarak da terbutalin sülfat kullandığı öğrenildi. Hastaya bu belirti ve bulgularla amoksisilin ile tetiklenen Kounis sendromu tanısı kondu. Tipik anaflaktik ve anaflaktoid belirti ve bulguların izlenmemesi eş zamanlı aldığı oral antihistaminik ve inhaler beta mimetik ajanlara bağlandı.
Akut koroner sendrom düşünülen hastalarda, öykünün derinlemesine araştırılması, doğru tanı konmasını, gereksiz girişimsel işlemlerden kaçınılmasını ve hastanın takip ve tedavisinin daha doğru şeklide yapılmasını sağlayacağı düşünülmektedir.
Turkish Keywords :
, Kounis sendromu
, Atipik
, Amoksisilin
Introduction
Cases of acute coronary syndromes occurring simultaneously with hypersensitivity reactions are called Kounis syndrome (KS). This syndrome was first described as allergic angina syndrome by Kounis and Zavras in 1991 1. Many allergic factors are described as the cause of KS 2-4. Although KS is a well-known entity in cardiology practice, many patients still cannot be diagnosed for various reasons. In our paper, we have discussed a 38-year-old male patient who had Kounis syndrome triggered by oral amoxicillin but who did not have the typical allergic symptoms because of the oral administration of clorpheniramine maleate and the inhaler terbutaline sulphate, which the patient was using at same time.
Case Report
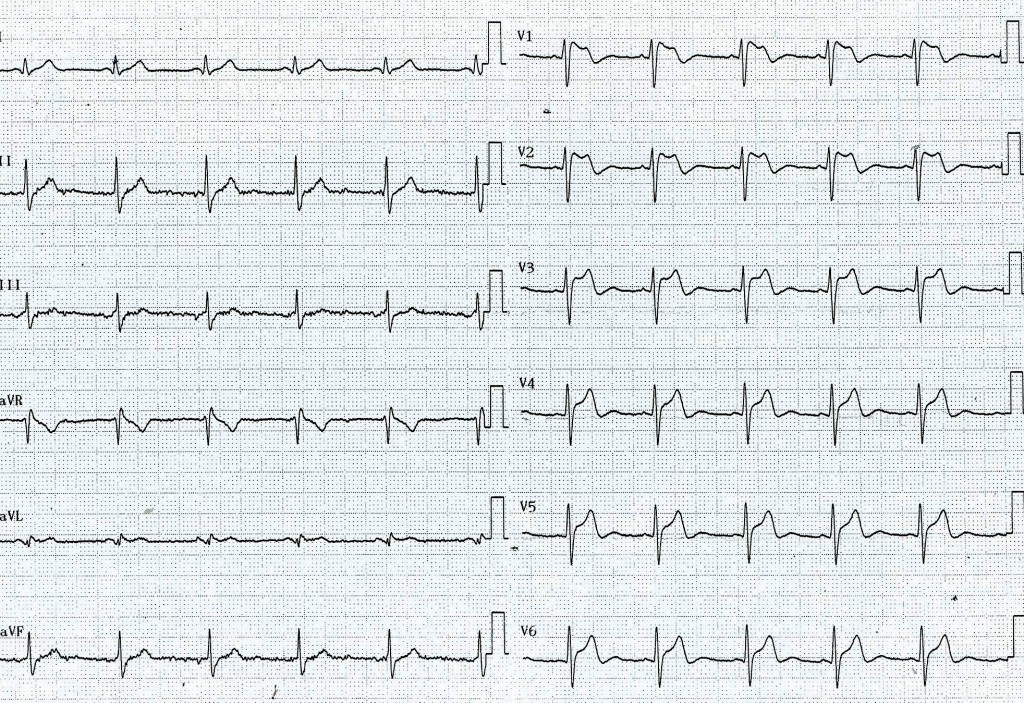
A 38-year-old male patient was admitted to the emergency department with dyspnea, nausea, and typical severe chest pain. The patient was experiencing these complaints for the first time. They lasted 30 minutes and the pain was referring to his back. At the first evaluation, the pain was continuous, his blood pressure was 100/60, and his heart rate was 70 bpm. On the ECG, there was ST segment elevation at precardial derivations, especially on V2- V3 (Figure 1).
With the diagnosis of anterior MI, 300 mg acetylsalicylic acid, 600 mg clopidogrel, 7500 IU unfractionated heparin, and 100 µg intravenous nitrate were given, and an immediate coronary angiography was performed. Normal coronary anatomy was detected. After the chest pain resolved, a new ECG was performed and the ST segment elevations had disappeared compared to the control ECG (Figure 2).
No pathology was detected through the transthoracic echocardiography. From the detailed anamnesis, it was learned that the patient was a heavy smoker and was using amoxicillin trihydrate 1000 mg, paracetamol 250 mg, oxolamine citrate 100 mg, and clorpheniramine maleate 2 mg orally and terbutaline sulphate as an inhaler for flu and cough. With these signs and symptoms the diagnosis was thought to be KS induced by amoxcillin. The lack of typical anaphylactic signs and symptoms were thought to be because of the oral antihystaminic and inhaler betamimetic drugs he used at the same time. At his follow-up, cardiac biomarkers did not increase. The patient was advised to quit smoking and 100 mg acetylsalicylic acid and 5 mg amlodipine treatment were started as he could not tolerate oral nitrate treatment.
Discussion
Today, many allergenic factors are known to cause of Kounis syndrome. These allergens are latex, snake poison, and some environmental factors like foods, antibiotics, anesthetic agents and medical interventions like drug eluting stents 2-4. During hypersensitivity reaction, mast cells are activated, coronary vasospasm occurs via proteases such as histamine, leucotrienes, and tryptase, and in some cases, this situation causes coronary plaque rupture, which triggers thrombus formation 5-7. Until now, three subtypes of KS have been defined. Type 1 occurs in patients without coronary atherosclerosis, type 2 occurs in patients with previous atherosclerosis, and type 3, which has been defined in recent years, occurs after drug eluting stent implantation 5-8.Apart from these, three clinical presentations are associated with KS. These are Takotsubo cardiomyopathy, coronary vasospasm at allogenic heart transplantation, and hypersensitivity-associated myocarditis 9, 10. In this patient?s case, there were ischemic ECG changes but there was no increase in cardiac biomarker readings. The clinical presentation did not progress to myocardial infarction. The patient had experienced this syndrome for the first time. This caused us to consider an underlying etiological cause. So, a detailed anamnesis was taken and amoxicillin treatment, which is often relevant with KS, was determined to be the probable cause. But, the diagnosis of KS was uncertain because of the absence of anaphylactoid signs and symptoms. It has been thought that the patient was using antihistaminic chlorpheniramine maleate and the inhaler terbutaline sulphate, which has beta mimetic and bronchodilator effects, so the allergic signs and symptoms were unclear. Clinicians should keep in mind that a detailed anamnesis of acute coronary syndrome will provide correct diagnosis, treatment, and follow for of patients and prevent unnecessary revascularization procedures.
References
- Kounis NG, Zavras GM. Histamine-induced coronary artery spasm: the concept of allergic angina. Br J Clin Pract. 1991; 45: 121-8
- Tavil Y, Turfan M, Turkoğlu S, et al. Kounis syndrome secondary to amoxicillin/clavulanic acid use. Int J Cardiol. 2008;124:e4-7.
- Almpanis G, et al. Kounis syndrome: two extraordinary cases. Int J Cardiol. 2011;147:e35-8.
- Venturini E, Magni L, Kounis NG. Drug eluting stent-induced Kounis syndrome. Int J Cardiol. 2011;146:e16-9.
- Kounis NG, et al. Kounis syndrome (allergic angina and allergic myocardial infarction). In: Gallo AP, Jones ML, editors. Angina pectoris: Etiology, pathogenesis and treatment. Hauppauge: Nova Science Publishers; 2008. p. 77-150.
- Fassio F, Almerigogna F. Kounis syndrome (allergic acute coronary syndrome): different views in allergologic and cardiologic literature. Intern Emerg Med. 2012;7(6):489-95.
- Schwartz LB. Diagnostic value of tryptase in anaphylaxis and mastocytosis. Immunol Allergy Clin N Am. 2006; 26: 451-63.
- Akyel A, et al. Late drug eluting stent thrombosis due to acemetacine: Type III Kounis syndrome Kounis syndrome due to Acemetacine. Int J Cardiol. 2012; 155: 461-2.
- Yanagawa Y, Nishi K, Tomiharu N, et al. A case of Takotsubo cardiomyopathy associated with Kounis syndrome. Int J Cardiol. 2009;132:e65-7.
- Biteker M, et al. Allergic myocardial infarction in childhood: Kounis syndrome. Eur J Pediatr. 2010;169:27-9.
|