Abstract
Aortic aneurysms (AA) diameter is the best predictor of rupture risk. Eccentric or saccular aneurysms has a greater rupture risk than more diffuse, cylindrical aneurysms. The endovascular treatment of thoracic aortic aneurysms (TAA) quickly gained an important role in current clinical management because of their less invasive nature, early recovery time and reduced perioperative morbidity as compared with open operations.
A case of huge 8-cm saccular descending aortic aneurysm in a patient receiving hemodialysis who was successfully treated with endovascular stent graft placement is reported. This study aimed to present an uncomplicated treatment of saccular aneurysm via endovascular technique in the descending aorta in a high-risk patient.
Keywords :
Saccular aneurysm
, Endovascular treatment
, Renal failure
Turkish Abstract
Aort anevrizmalarında (AA) çap, rüptür riski için en iyi prediktördür. Egzentirik veya sakküler anevrizmalarda rüptür riski, difüz ve silindirik anevrizmalara göre daha yüksektir. Torasik aort anevrizmaların (TAA) endovasküler yöntemlerle tedavisi, açık cerrahi yöntemlere göre, erken nekahat, düşük preoperative morbidite ve mortalite oranları nedeniyle klinikte hızla önemli bir yer kazanmıştır.
Hemodiyaliz alan bir hastada 8 cm olan sakküler desendan aort anevrizması, endovasküler stent grefti ile başarıyla tedavi edilmiştir. Bu çalışma ile yüksek riskli bir hastada sakküler anevrizmanın, endovasküler teknik kullanılarak başarı ile tedavisinin gösterilmesi amaçlandı.
Turkish Keywords :
, Sakküler anevrizma
, Endovasküler tedavi
, Böbrek yetmezliği
Introduction
Descending thoracic aortic aneurysms may be treated with open surgical repair techniques and may carry low morbidity and mortality if the experience of the surgeon and operative technique is proper. On the other hand, thoracic endovascular aortic repair is less invasive and easy to perform. Anatomy, pathology of the aorta and proximity of major branches are the limitations of endovascular procedures. Although the endovascular management of these patients seemed to be complex and technically demanding, traditional open surgery has a higher perioperative risk and redo procedures require a high level of expertise skill 1. Saccular aortic aneurysms have always been a matter of concern for the surgeons because of the general belief that their unique shape predisposes them to rupture. Surgical repair is indicated for symptomatic and asymptomatic saccular aneurysms 2. The objective of this report is to present a huge saccular aneurysm and endovascular management of this uncommon pathology in a patient who has been receiving hemodialysis therapy for the recent 6 years due to chronic renal failure.
Case Report
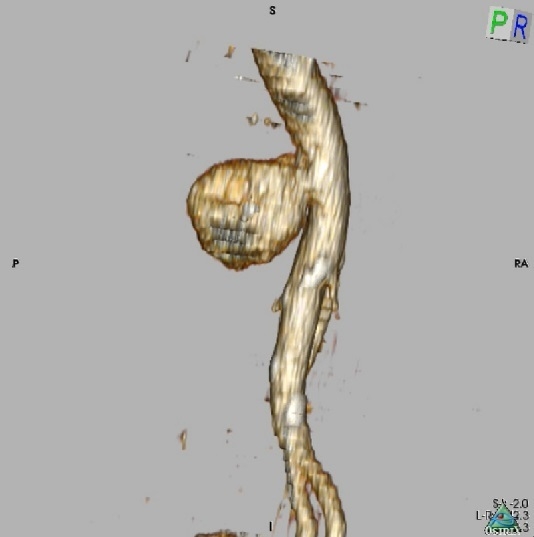
A 64-year-old woman receiving dialysis therapy was referred to our institution after the incidental discovery of an 8 cm saccular descending aortic aneurysm. The diameter of the descending thoracic aorta proximal and distal to the aneurysm was 27mm and 26mm respectively. The computed tomography (CT) revealed an aneurysm involving the descendan proximal abdominal aorta which ends at 3 cm superior to the celiac artery (Figure 1).
The patient?s medical and surgical history was significant for chronic renal failure and a hysterectomy through a midline laparotomy. Transthoracic echocardiography revealed wall motion abnormalities of the left ventricular apex with an ejection fraction of 30%. In light of the significant concern for the development of low cardiac output symptoms and heart failure a conventional repair was considered to be a very high risk. Stent-graft placement was discussed with the patient. The patient agreed to undergo this procedure and written informed consent was obtained.
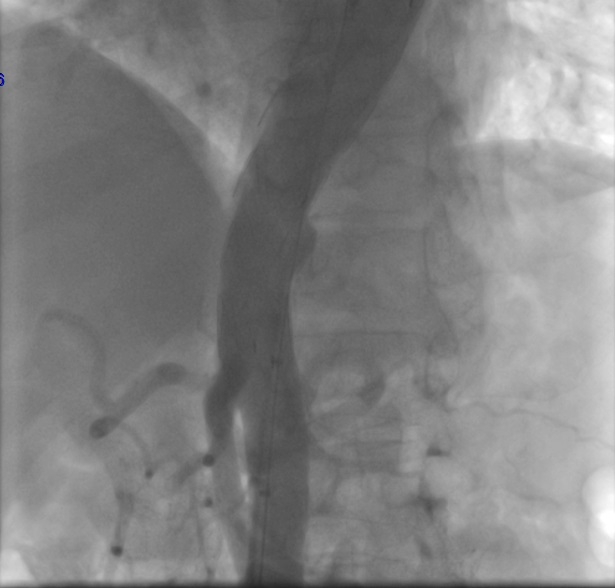
Under local anaesthesia and sedation, right femoral artery was exposed. A 6 French pigtail catheter was inserted via the left femoral artery and hydrophilic guide wire were advanced to arcus aorta to localize the site of aortic branches. The rigid guide wire inserted through right femoral artery. Arteriotomy was performed to right femoral artery. The thoracic stent-graft 30mm x 150mm Bolton relay NBS plus (Bolton Medical, Sunrise, FL, USA) was advanced to the descending aorta. The stent-graft was deployed distally to the left brachial artery and proximal to the coeliac trunk. The control angiography revealed type I endoleak from the distal attachment site. A balloon dilatation was performed to distal end of aneurysm. Repeated control angiography showed resolution of the type I endoleak (Figure 2).
The patient?s initial recovery was uneventful. The patient was discharged on the 4th day after the procedure. No complications have been identi?ed during regular follow-up.
Discussion
There is a common perception of a more malignant natural history of saccular aortic aneurysms than fusiform aneurysms but the true rupture risk of saccular aneurysms is actually unknown. Aneurysm growth rate and the diameter is considered the major determinant for rupture risk 3. While numerous other studies implicate also aortic asymmetry as a proxy for rupture risk and aneurysm growth 4. Maier et al examined the natural history of aort aneurysms and compared them for their diameter, wall stress, and rupture potential. They showed that neither aortic diameter nor other measured saccular aneurysm diameters predicted aneurysm growth. They stated that the heterogeneity of the detected growth rates suggests that individual aneurysm characteristics may be important in determining aneurysm stability 5.
Open surgical repair of saccular descending aortic aneurysms is the recommended treatment option in patients with surgically acceptable risk. In high-risk patients, however, an alternate endovascular option should be strongly considered 6. Surgical and endovascular risk assessment was discussed with the patient. Our patient agreed to underwent an endovascular procedure. Even though, early complication rates are low after endovascular procedures complications such as endoleak, stent migration and paraplegia may occur. Endoleak may be diagnosed at the time of stent deployment. İn our case we detected a distal type I endoleak at the control angiography performed after graft implantation. Endoleak was successfully repaired by balloon dilatation and control angiographic was normal. CT scans at 3rd month showed complete healing of the aortic wall. The patient planned to follow with serial CT to look for endoleak, stent migration or aneurysm in the postoperative period.
In conclusion, endovascular procedure can be selected as a treatment option for giant saccular aneurysm in surgically high risk patients. However, long-term prognosis of the treatment depends upon the aneurysm characteristic and the stability of the endovascular stent. Long-term follow-up is necessary to establish the efficacy of this treatment option.
Acknowledgement
?The authors declare that the research was not carried out with the financial support (or other form of support) of a governmental institution, pharmaceutical company, foundation, private enterprise, or governmental enterprise.?
?All authors declare that there is no conflict of interests regarding the publication of this article.?
References
- Fehrenbacher JW, et al. Early and late results of descending thoracic and thoracoabdominal aortic aneurysm open repair with deep hypothermia and circulatory arrest. J Thorac Cardiovasc Surg. 2010 ;140(6 Suppl):S154-60.
- Taylor BV, Kalman PG. Saccular aortic aneurysms. Ann Vasc Surg. 1999 ;13(6):555-9.
- Shang EK, et al. A modern experience with saccular aortic aneurysms. J Vasc Surg 2013; 57(1): 84-8.
- Nathan DP, et al. Increased wall stress of saccular versus fusiform aneurysms of the descending thoracic aorta. Ann Vasc Surg 2011;25:1129-37.
- Maier A, et al. A comparison of diameter, wall stress, and rupture potential index for abdominal aortic aneurysm rupture risk prediction. Ann Biomed Eng. 2010;38:3124-34.
- Uğur M, et al. Vasküler hastalıkların yönetiminde endovasküler ve hibrid uygulamalar: Kardiyovasküler cerrahi kliniği deneyimleri. Turk Gogus Kalp Dama. 2012;20(2):230-42. doi: 10.5606/tgkdc.dergisi.2012.046.
|