Abstract
A 22-year-old woman, who was diagnosed atrial septal defect, was treated with an Atrial Septal Occluder (ASO) device after routine cardiological examination. After 24 hours, she had an urgent operation with diagnose of the embolized ASO device. Herein, we are reporting a case of left pulmonary artery embolization of ASO device and want to highlight the patient selection for this procedure.
Keywords :
Atrial septal defect
, Septal occluder device
, Pulmonary embolism
, Cardiac surgical procedures
Turkish Abstract
Atrial septal defect tanısı konulan 22 yaşındaki kadın hasta, rutin kardiyak değerlendirme sonrasında atrial septal tıkaç cihazı ile tedavi edildi. İşlemden 24 saat sonra atrial septal tıkaç cihazının embolisi nedeni ile acil operasyona alındı ve cerrahi ile başarılı bir şekilde tedavi edildi. Bu yazıda atrial septal tıkaç cihazının sol pulmoner artere embolizasyon sonrasında tedavi edilmesi sunularak hasta seçiminin önemi vurgulanmaktadır.
Turkish Keywords :
, Atrial septal defekt
, Septal tıkaç cihazı
, Pulmoner emboli
, Kardiyak cerrahi prosedür
Introduction
Various devices have undergone clinical trials of transcatheter closure of atrial septal defects (ASD) in which concerns related to large delivery systems, complicated delivery techniques, fatigue fractures of metal struts, device displacement, or perforation of atrial wall have been addressed. With the worldwide experience growing steadily with the Atrial Septal Occluder (ASO), it has assumed an enviable position in the nonsurgical transcatheter closure of ASD and other interatrial communications. In our limited experience of a case with ASO, we highlight the consideration about case selection.
Case Report
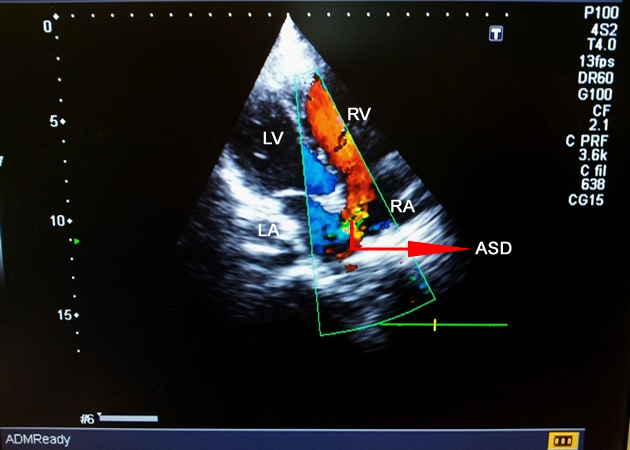
A 22-year-old girl presented with history of palpitations and breathlessness of one years? duration. Clinical examination favored diagnosis of an ASD with left-to-right shunt greater than 2 : 1. Transthoracic echocardiography (TTE) using multiple subxiphoid and precordial views confirmed the diagnosis and delineated the morphology of the ASD. Transesophageal echocardyography (TEE) performed and fossa ovalis defect measured 18 mm, and the septal rim was at least 10 mm from the right pulmonary veins, superior vena cava, ostium of coronary sinus, and mitral valve. But aortic rim measured 2 mm.These rim sizes considered as suitable for an ASO, although septum was floppy and mobile. The patient underwent cardiac catheterization. ASD closed with ASO (Figulla Flex, Occlutech, Helsingborg, Sweden) described previously 1. After confirmation of the position and stability of the device on fluoroscopy and TEE, it released. After the procedure, the patient monitorized at the coronary intensive care unit. After 24 hours, suddenly the patient developed palpitation, agitation, epigastric pain and vomitings accompanied by severe retching. Cardiac auscultation revealed evidence of left-to-right shunt as before, which prompted an urgent TTE. TTE revealed that the ASO displaced from the atrial septum and embolized to the main pulmoner artery and lokalized like a plug through the left pulmonary artery (Figure 1-a and 1-b).
Low moleculer weight heparin (enoxaparine) administered 0.1 ml/kg IV (0.7 ml, IV) and the patient sent to open heart surgery. Surgical procedure was performed by the standard method, which included a median sternotomy, the opening of the pericardium. The patient was put on cardiopulmonary bypass (CPB) by aorta-bicaval cannulation, and the heart stopped by anterograde cardioplegia. The presentation of the interatrial septum performed through the right atrium.The ASO device was tried to pull through the right ventricule with finger maneuver but failed wherein retrieved through the main pulmonary artery from an approach of 2 cm oblique arteriotomy. The wire mesh of the polyester-filled prosthesis was partially invested by a layer of organizing fibrin, but there were no thrombi on the surface of the retrieved device and on close examination it appeared to be structurally intact (Figure 1-c).
The ASD was oval in shape, measured 15 x 8 mm, and had intact rims all round while infero-anterior rim was thin and flowing. The ASD closed with continuous nonabsorbable prolene sutures. Right atriotomy sutured with nonabsorbable prolene sutures. After heart started to beat, weaned from the CPB, and the surgery finished by standard method without any complication. The patient made an uneventful recovery and discharged 5 days after operation and 6 mount follow up was smoothly.
Discussion
The ASO is a self-centering prosthesis with the advantage of having a smaller overall size. The overall placement technique appears simpler than with other existing devices and hence has a shorter learning curve. The ASO closes the ASD by stenting the defect with its conjoint waist. However, patient selection needs to be appropriate, especially with respect to morphology of the defect, its stretched diameter, surrounding rims and structure of the septum 1. Oval defects are liable to be undersized as resistance from the minor diameter may be felt as the balloon is withdrawn across the defect. This error is minimized by adopting the use of TEE. The right atrial retention disc of ASO is made slightly smaller than the left, taking into account the uniformly present left-to-right transatrial pressure gradient. Device dislodgment can occur if the size of the defect greatly exceeds the waist diameter of the device or approaches the diameter of the retention discs 2. Another cause of dislodgment is instable placement of ASO by an incomplete ring of rim. Young et al 3 reported an embolization of ASO to the main pulmonary artery (PA) which occurred overnight and was managed surgically without any further complications. When re-examination of the patient during the surgery they have observed that patient had a large anteriorly placed ASD through which the superior aspect of left-atrial disc prolapsed into the right atrium and subsequently migrated into the PA. As in this case while the infero-anterior rim was thin and floppy, TEE or TTE should pass over these details.
On the other hand, placement of a disproportionately large device may result in mushrooming of the retention discs and weakening of the cross-clamping forces against the septal rim, which increases the risk of blood flow behind the discs and may result in incomplete endothelialization.
Amanullah et al 4 was reported device embolization within minutes of release. This pattern of early device embolization necessitating surgical intervention finds mention in recent literature as well 1. Acute device failure is usually secondary to poor case selection or device selection (low device-defect ratio), operator-related failure, inaccurate deployment, inadequate defect rim to hold the device, and tearing of the interatrial septum, especially at the lower rim of the ASD owing to excessive catheter and device manipulation 5-6.
We have an urgent open heart operation in this ASO device embolization because it was obstructing blood flow through the main pulmonary artery to the left pulmonary artery. Although the device was impacted in a high-blood-flow velocity zone, we preferred to administer low molecular weight heparin to the patient before surgery in order to prevent potential thromboembolic complications. The sequela of device embolization is likely to be ominous and hence necessitates urgent intervention.
Conclusion
This case is being reported to highlight the following: 1- Early embolization of a mechanically intact ASO, likely in a setting of a delicately straddled device getting dislodged by instable placement to the incomplete ring of rim; 2- The importance of performing a preprocedural TEE in multiple views to assess preoperatively the morphology of the ASD with respect to its location, size, shape, margins and nature of rim; 3- The drawback of balloon sizing in oval-shaped septal defects, especially if not complimented with TEE; 4- The need for surgical intervention in practically every patient to retrieve the errant device. These facts may be well known to an experienced operator, but for a new entrant in this field, it is important to realize that the technical and clinical success of this procedure largely depend on meticulous case selection.
References
- Gadhinglajkar S, et al. Surgical retrieval of embolised atrial septal occluder device from pulmonary artery: Pathophysiology and role of the intraoperative transoesophageal echocardiography. Annals of Cardiac Anaesthesia. 2009:12:140-48.
- Duygu H, et al. Silent embolization of an Amplatzer atrial septal closure device into the main pulmonary artery: Pivotal role of routine postprocedural surveillance echocardiography. International Journal of Cardiology. 2011;148(2):235?7.
- Young HK, et al. Emergent surgical intervention for embolization of atrial septal defect closure device. Korean J Thorac Cardiovasc Surg. 2012;45:320?2.
- Ferrero E, et al. Migration of an AMPLATZER a trial septal occluder to the abdominal aorta. The Am J Cardiol [Internet]. 2013;112(4):612?3.
- Amanullah MM, et al. Surgical rescue of embolized amplatzer devices. J Cardiac Surg. 2011;26(3):254?8.
- Godart F, et al. Experience in one centre using the buttoned device for occlusion of atrial septal defect: Comparison with the Amplatzer septal occluder. Cardiol Young. 2000;10:527-33.
Information Presentation
Türk Kalp Damar Cerrahisi Ulusal Kongresi 2012, Poster Bildirisi, Antalya
|