Abstract
Sigmoid volvulus frequently presents in elderly at the seventh and eighth decades and may occur due to colonic cancer. Volvulus is rare in adolecents, and when occurs the diagnosis may be delayed. We report an adolescent with volvulus of the sigmoid colon without any previous abdominal procedure. The etiology was dense adhesions throughout the whole abdominal cavity running along the sigmoid mesentery. The patient was treated with sigmoid resection and primary anastomosis.
Keywords :
İntestinal volvulus
, Adolescent
, Colon
Turkish Abstract
Sigmoid volvulus sıklıkla, 70?li 80?li yaşlardaki yaşlılarda kolon kanserine bağlı gelişen bir tablodur. Volvulus gençlerde nadirdir ve geliştiğinde genellikle tanı geç konulur. Bu olguda daha önce abdominal cerrahi öyküsü olmayan ve sigmoid kolon volvulusu gelişen genç bir hastayı sunduk. Etyolojik faktör; sigmoid mezenteri çevreleyen ve tüm abdominal boşlukları tutan yoğun adezyonlar idi. Hasta sigmoid rezeksiyon ve primer anastomoz ile tedavi edildi
Turkish Keywords :
, İntestinal volvulus
, Genç
, Kolon
Introduction
Sigmoid volvulus is a closed loop obstruction usually due to a twist around a short mesenteric root. The condition is frequent in seventh and eighth decades 1 and usually associated with chronic constipation. The most important and most common etiologic factor that has to be considered in adults is (65%) neoplasms. Other common causes include adenopathy, polyps, diverticulitis and trauma 2. But in childhood the most common etiologic factors are malrotation, Meckel?s diverticulum, meconium ileus, mesenteric cysts, duplication cysts, jejunal atresia or stenosis 3. The early diagnosis is vital in all cases because misdiagnosis may lead to disastrous complications such as bowel ischemia, strangulation, gangrene and perforation. The mortality rate is noted high (%33-80) 2,4.
Altough physicians are familiar with this clinical situation in elderly patients, the acute peritoneal symptoms accompanied by severe distention of the abdomen and constipation in young patients are also prominent. Volvulus of the sigmoid colon typically presents with severe abdominal pain with acute onset accompanied with ongoing constipation, distention, nausea and vomiting. Radiologic studies and blood count are used in diagnosis. White blood cell count may not be increased in all patients but in plain abdominal films several signs from mild to severe may be seen. The radiologic findings vary from non specific air-fluid levels, enlarged colonic gas images due to colonic dilatation to ?coffee-bean? sign which is pathognomonic for sigmoid volvulus 5.
Case Report
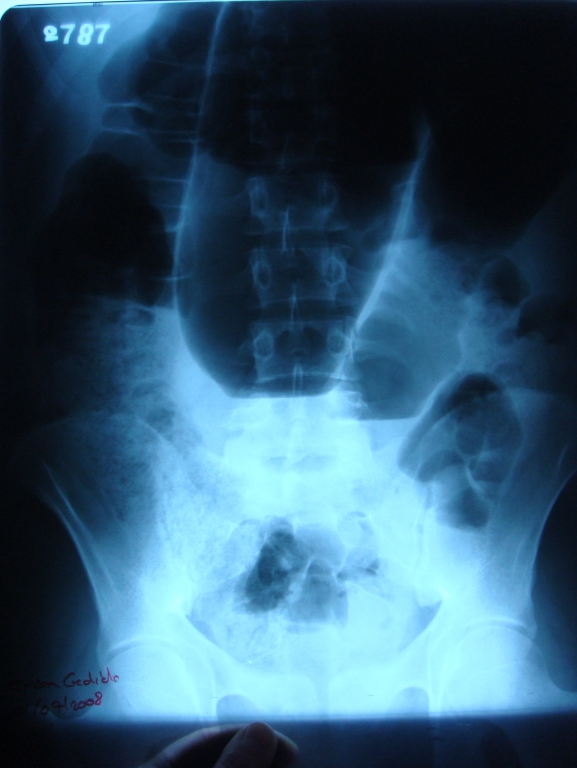
A 17 year old male patient presented to our outpatient clinic with mild abdominal pain, constipation without nausea, vomiting and severe abdominal distension. The patient had no abdominal operation before and he denied previous bout of constipation. The complaints had started two days earlier and the patient?s oral intake was normal. The physical examination was normal except severe abdominal distention and hypoactive bowel sounds. Digital rectal examination was normal except empty ampulla. No blood was present in distal rectum. Laboratory parameters were totally in normal ranges. An upright plain abdominal film revealed the distended sigmoid colon with ?coffee-bean? sign (Figure 1).
Rigid rectosigmoidoscopy failed to decompress the distended sigmoid loop thus we proceeded with laparotomy. Laparotomy revealed a distended sigmoid loop over 20 cm at the largest segment with a dense adhesions on the root of the mesentery (Figure 2).
Abdominal exploration revealed accompanying dense adhesions all around the abdominal cavity, especially around the ceacum. Sigmoid resection and primary anasthomosis was performed because no signs of bowel ischemia was seen. No further action was taken for adhesions in other parts of abdominal cavity.
Discussion
Sigmoid volvulus may be a disastrous problem both in elderly and young ages when misdiagnosed because of the risk of bowel ischemia leading to strangulation, perforation and peritonitis. Although in elderly period the diagnosis is easily considered, and an underlying process like chronic constipation, previous diverticulitis attacks and adhesions due to previous operations are usually present; the children and young adolescents are disadvantaged under these circumstances because it may easily be misdiagnosed. According to the stage of the process the symptoms and findings may vary in a wide spectrum; plain abdominal films may relieve air-fluid levels which are not specific to volvulus but may be seen in a large variety of disorders which cause colonic obstruction. Patients may not have any pathologic laboratory findings. Even during an ongoing obstructive process patients may have stool in rectum and/or normal oral intake as in our case which may prevent the surgeon from early diagnosis.
The ?coffee-bean? sign which is formed by the upper limb of the gas-filled sigmoid loop as a large inverted ?U? with a fluid level in each limb in plain abdominal radiographs and ?bird?s beak? sign in water-soluble contrast enema study 6 are diagnostic for sigmoid volvulus and no further radiologic investigation is necessary. Use of computed tomography (CT) in the diagnosis of sigmoid volvulus is controversial. In a great variety of cases the clinical presentation is typical and plain upright abdominal radiograms reveal clearly the pathognomic signs . Therefore, when the young adolescents and children are considered CT is crucial in the algorithm. In our case, plain upright abdominal radiogram revealed the coffee-bean sign and the diagnosis was clear. No further investigation was needed to decide the therapy. But in elderly patients a CT scan may be included in order to verify any possible underlying colonic malignancy. Besides eliminating the malignancy, CT scan can reveal the adhesions at the mesentery of the sigmoid colon known as the ?whirl? sign 5, but it is not as pathognomic as the coffee-bean sign or bird?s beak sign.
After the diagnosis is clear and any malignancy is eliminated first step in the algorithm should be endoscopic decompression. We also tried endoscopic decompression in the operation room with a rigid proctoscope but failed. The effectiveness of endoscopic decompression is 81% but it also has a recurrence rate between 55% and 90% 7 , and the patients usually have to have a laparotomy in order to resect the long sigmoid loop. Endoscopic decompression should be thought as a palliative initial step of the algorithm in order to prevent the patient from an emergency laparotomy and increase the primary anastomosis chance at the same time. Considering that a long sigmoid loop is the prior reason underlying the problem, the resection of this segment is for sure the exact therapy. After the failure of the endoscopic decompression the patient is prepared for a laparotomy immediately in the operation room. The aim is to resect the long sigmoidal loop and primary anastomosis should be done if no sign of bowel ischemia is seen. We performed stapled primary anastomosis after sigmoidal resection. If the assessment of the bowel wall reveals that a primary anastomosis will not be safe, a temporary colostomy or diverting loop ileostomy should be done.
Sigmoid volvulus is a frequent clinical situation and the diagnosis may easily be cleared with basic physical examination and simple radiographic studies. These would be either a plain upright radiograph or a water-soluble contrast enema study; the latter being both diagnostic and therapeutic. CT should be considered in elderly cases in order to eliminate the possibility of the underlying colononic malignancy. The first step of the algorithm is endoscopic decompression and one should remember that the technique itself is a palliation to prevent the emergency laparatomy and enhance a primary anastomosis. Considering that the underlying cause is the long sigmoid loop the surgical therapy should consist a sigmoid resection.
References
- Lou Z, et al. Appropriate treatment of acute sigmoid volvulus in the emergency setting. World J Gastroenterol. 2013;14:4979-83. doi: 10.3748/wjg.v19.i30.4979.
- Katsikogiannis N, et al. Management of sigmoid volvulus avoiding sigmoid resection. Case Rep Gastroenterol. 2012;6:293-9. doi: 10.1159/000339216. Epub 2012 May 23.
- Valsdottir E, Marks JH. Volvulus: small bowel and colon. Clin Colon Rectal Surg. 2008;21:91-3. doi: 10.1055/s-2008-1075856.
- Salinas NL, et al. A surprising twist to an old problem: Sigmoid volvulus in a 19-year-old man. Am Surg 2007;73: 284-6.
- Salati U, McNeill G, Torreggiani WC. The coffee bean sign in sigmoid volvulus. Radiology. 2011;258:651-2. doi: 10.1148/radiol.101882.
- Moore CJ, Corl FM, Fishman EK. CT of cecal volvulus: unraveling the image. AJR Am J Roentgenol. 2001;177:95-8.
- Hougaard HT, Ovist N. Elective surgery after successful endoscopic decompression of sigmoid volvulus may be condisdered. Dan Med. J. 2013; 60: A 4660.
|