Abstract
Endometriosis is defined by the presence of functional endometrial tissue outside the uterus. The rectus abdominis muscle is an uncommon site of extrapelvic endometriosis, which usually develops in a previous surgical scar and it should be considered in the differential diagnosis of any abdominal swelling. Incisional endometriosis should be considered among the diagnoses if the patient defines cyclic pain in yhe masses emerging on the previous ceasarian scarring. In this case, we aimed to present the findings of ultrasonography, computerized tomography, magnetic resonance imaging and microscopic and macroscopic pathological findings of a patient, being diagnosed to have rare endometriosis on rectus abdominis together with the present literature.
Keywords :
Abdominal wall
, Cesarean section
, Endometriosis
, Rectus abdominis muscle
, Scar endometriosis
Turkish Abstract
Endometriozis, fonksiyonel endometrial dokunun, uterus dışında bulunması olarak tanımlanmaktadır. Ekstrapelvik endometriozisde, rektus abdominis kas yerleşimi çok sık görülmemekte olup, genellikle önceki cerrahi skardan gelişmektedir. Sezeryan skarında gelişen kişilerde, hasta siklik ağrı tarif ediyor ise, insizyonel endometriozis, ayırıcı tanılarda düşünülmelidir. Bu olgu sunumunda, nadir görülen, rektus abdominis kasında endometriozis tanısı alan hastanın ultrasonografi, bilgisayarlı tomografi, manyetik rezonans görüntüleme bulgularını, mikroskopik ve makroskopik patolojik bulgularını, mevcut literatür bilgileri eşliğinde sunmayı amaçladık.
Turkish Keywords :
, Abdominal duvar
, Sezeryan kesisi
, Endometriozis
, Rektus abdominis kası
, Skar endometriozisi
Introduction
Endometriosis is defined by the presence of functional endometrial glands and stroma outside of the uterine cavity 1. Endometriosis is one of the most common gynecologic entities, present in 8%-18% of menstrual woman 2. Endometriosis can occur at intrapelvic and extrapelvic localizations.Most commonly, intrapelvic endometriosis is observed. Extrapelvic endometriosis may develop in any organ including the skin, lungs, liver, extremities, brain and stomach. Endometriosis of the abdominal wall is a subtype of extrapelvic endometriosis and is uncommon. Usually presentation includes palpable mass, cyclic pain during the menstruation, bleeding and discharge. Endometriosis involving the rectus abdominis muscle is rare.Generally, there is a history of an operation like a ceasarian section or hysterectomy 1. The incidence of endometriosis on the site of incision after ceasarian section is between 0.03-0.4% 3. Differential diagnosis includes abscess, lipoma, hematoma, sebaceous cyst, suture granuloma, inguinal hernia, incisional hernia, desmoid tumor, sarcoma, lymphoma and primary or metastatic cancer 4. Endometriosis has no pathognomonic imaging findings on computer tomography (CT), magnetic resonans imaging (MRI) or ultrasound (US) as its appearance depends on the phase of the menstrual cycle, the proportion of stromal and glandular elements, the amount of bleeding and the degree of surrounding inflammatory and fibrotic response 5.
In this case, we presented a patient with history of a ceasarian section, who was diagnosed to have localized endometriosis on rectus abdominis muscle and over the ceasarian scarring.
Case Report
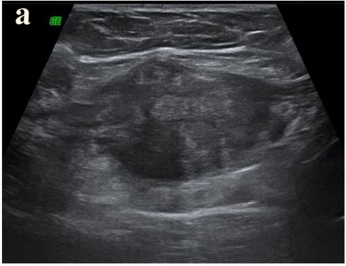
A 22 year-old female patient was attended to our hospital because of pain in right lower quadrant of abdomen lasting for a year, which increased in latest months. We learnt from the patient's history that the pain was related to the menstruation and and there had been a swelling bulging during menstruation over the scarring on right lower quadrant of the abdomen. Her cycles were regular and painless. She had a ceasarian section 21 months ago in her medical history. During the physical examination, there was no other special finding other than the tenderness over the right lateral of ceasarian incision. No remarkable difference was detected in routine blood count and the biochemical tests. Abdominal ultrasonography was normal and the uterus and the ovaries were observed normal the pelvic ultrasonograhy. A hypoechoic, localized mass with irregular contours, which is 45x37x24 mm in dimensions was observed within the rectus abdominis muscle under the right lateral of the incision line during the superficial ultrasonographic examination. Vascular signalling, being more prominent on the periphery of the mass was present during the Doppler ultrasonograhy examination (Figure 1a, 1b).
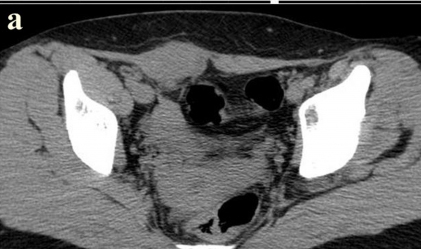
The mass had no association with the intraabdominal organs. Because of the irregular contours of the mass and to detect the rims clearly and to investigate the additional pathologies pelvic CT and MRI were carried on. İv contrast medium could not be infused due to the previous history of allergy for the contrast agents.The abdominal computerised tomography scan demonstrated a subcutaneous, extra fascial mass which was localised to the right side of the midline, at the medial edge of the right rectus abdominus muscle sheath(Figure 2a).
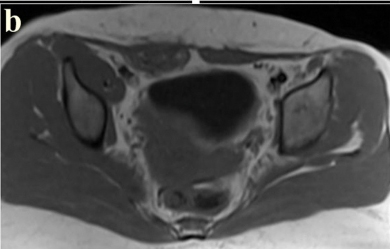
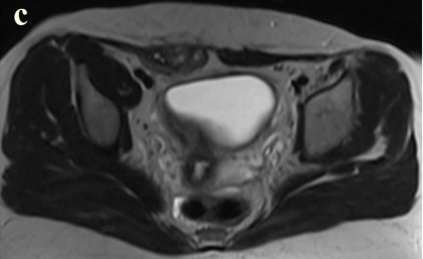
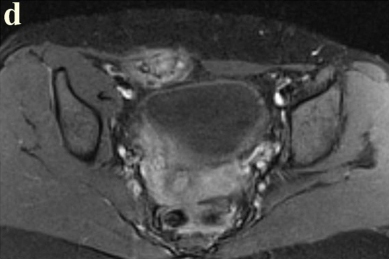
During the contrasted and non-contrasted pelvic MRI, a mass within the rectus abdominis muscle in the right lower quadrant of the abdomen, which was slightly hyperintense on T1-weighted sections and hyperintense on T2-weighted sections was observed. There had been milimetric nodular hemorrhage areas within the mass, which were hyperintense on T1 and T2-weighted sequences. Axial T1 weightedfat-saturated image after intravenous gadolinium contrast medium administration showing marked but inhomogeneous contrast enhancement of the mass in the right lower rectus abdominis muscle(Figure 2b-d).
The radiographic features suggested either endometriosis or desmoid. Under sterile conditions, after local anesthesia, US-guided, with14-gauge core biopsy needle, 2 blocks tru-cut biopsy was perform from the mass(Figure 1c).
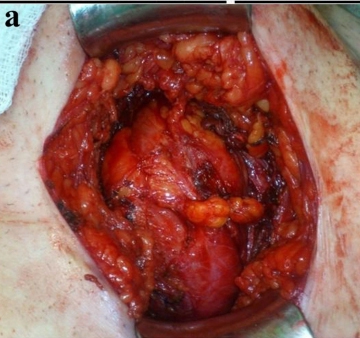
Histopathological analysis of the tissue revealed a large number of endometrial glands and stromal components. Microscopic examination of the mass confirmed endometriosis. The patient underwent surgery without any medical treatment.The operation was performed under general anesthesia. At surgery vascular mass in the right rectus muscle incision scar and surrounding normal tissue were removed, complete with a wide surgical excision.Grossly the mass consisted of highly vascular and fibrotic tissue (Figure 3a).
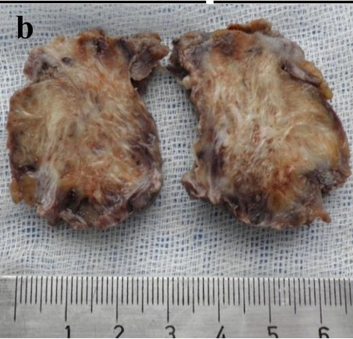
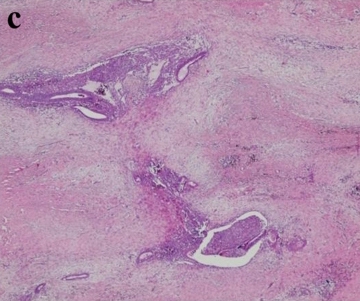
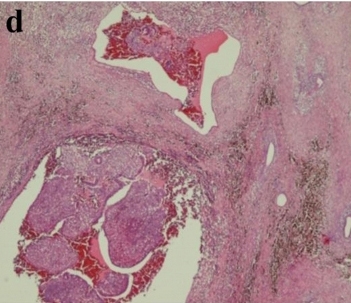
The histopathological and macroscopic examination showed the presence of endometriotic tissue(with small glands containing adjacent endometrial stroma)within the fibroadipose and the muscle of the abdominal wall, surrounding fibrosis, was removed with clear surgical resection margins(Figure 3b-d).
The patient was discharged on the second day after surgery. Control of the patient's examination was normal during the first, third and sixth postoperative months, there was no complaint.
Discussion
Endometriosis was first defined in 1900 6. Endometriosis, is a common gynecological disease with an estimated prevalence of 8?15% 7. The extrapelvic implantations of endometrial tissue were detected in various organs and systems (bladder, kidney, bowel, omentum, lymph nodes, lungs, pleura, extremities, umbilicus, hernial sacs) and the abdominal wall 8. Endometriosis involving abdominal wall especially into the rectus abdominis muscle is a rare site of extrapelvic endometriosis localization, usually reported in a previous surgical scar. In cases of abdominal wall endometriosis is 4% of all cases of external endometriosis 1. Several theories have been proposed for the development of extrapelvic endometriosis including retrograde menstruation, metaplasia, venous or lymphatic metastasis and mechanical transplantation into the scars at the time of surgery 9-11. During a caesarian section, endometrial tissue may escape through the incision in the uterus and implant themselves within the abdominal Wall 10,12. The tissue either proliferates under the same hormonal influences as endometrium in utero or induces metaplasia of the surrounding fascial tissue to form an endometrioma 13. The incidence of developing endometriosis over the incision scar is related to the the indication of hysterotomy. The incidence of endometriosis on scarring is 5.08% after hysterotomy due to second trimertes abortuses while it is varying between 0.03%-0.4% after ceasarian section 14. Common presentations include palpabl mass, cyclic pain and bleeding consecutively. Pain is the most common presenting symptom. The ectopic endometrium responds to the cyclic hormonal changes of the woman and bleeds into surrounding stroma causing pain from pressure. Endometriosis pain has generally been described as cyclical; however many reports in literature frequently refer no cyclic symptoms in association with abdominal wall location, thus making it difficult to make a preoperative diagnosis 15. The detection of painful nodules on the site of incision, changing with the menstrual cycle, which is the classical clinical finding in cases of ceasarian section endometriosis easily demonstrates the preoperative diagnosis 16. In our case, similarly, there was a painful mass on the site of incision, which becomes remarkable during the menstrual cycles with increasing pain. The literature emphasizes that scar endometriosis is uncommon; however, it may occur more commonly than believed. Time interval between operation and presentation scar endometriosis has varied from 3 months to 10 years in different series 16-18. Our patient had a history of cesarean section 21 months ago, pain in ceserean section scar had begun nine months after the operation.
Scar endometriosis is difficult to diagnose with physical examination. It is often misdiagnosed as granuloma,incisional hernia, inguinal hernia, hematoma, lymphadenopathy, lymphoma, lipoma, abscess, subcutaneous cyst, neuroma, soft tissue sarcoma, desmoids tumor, or even primary and metastatic cancer 7,19. Endometriosis of the abdominal wall can be visualized by US, CT or MRI. But endometriosis has no pathognomonic imaging findings on ultrasound, CT nor MRI, as its appearance depends on the phase of the menstrual cycle, the proportion of stromal and glandular elements, the amount of bleeding, and the degree of surrounding inflammatory and fibrotic response 5,20. Ultrasound, CT, and MR imaging may be used to depict an endometriotic lesion, exclude endometriosis, or provide evidence for an alternative diagnosis.
In cases of endometriosis seen on the abdominal wall, there can be cystic, polycystic, mixed and solid images sonographically 21,22. Demonstration of cystic areas within the solid mass, having irregular contours and receiving vascular signals from the mass during Doppler examination are in favor of endometriosis. In our case, the mass was solid with irregular contours and it was located within the rectus muscle. There was vascular signalling within the mass and on its periphery during Doppler examination. With these findings, hernia, lymphadenopathy, lymhoma, abscess and subcutaneous cyst were excluded.
CT and MR imaging findings of abdominal wall endometriosis are nonspecific also, both usually showing a solid enhancing mass in the abdominal wall. The major role of CT and MRI may be to depict the extent of the disease preoperatively, detecting the planes between muscles and abdominal subcutaneous tissue 23. MR is highly sensitive in detecting very small masses and offers excellent differentiation of endometriomas from neighbouring tissue 24. MRI can be more helpful especially when the lesion is small because of its high spatial resolution 23.
In some cases we can see classical MRI findings are consisting of multiple cystic structures which appear hyperintense on T1 weighted images and having different signal intensity patterns on T2 weighted images. The high proportion of glandular tissue also might explain the moderate to high contrast enhancement on MRI. In particular, the presence of blood products in an anterior abdominal wall mass at MRI with no other explanation is strongly suggestive of scar endometriosis 4,22,23. For this reason, in diagnosis of endometriosis, MRI is superior to US and CT 4,23.Our case was performed with noncontrast CT because of a history of allergy to contrast material. The mass was seen to be located within the rectus muscle on CT. Hyperintense foci of haemorrhage within the mass were observed on MRI.
Due to this non-specific imaging findingsa certain diagnosis can only be accomplished by histological examination of the lesion (fine-needle aspirate or core biopsy obtained under ultrasound or CT-guidance)5as was the case in our patient. Using fine needle aspiration biopsy for diagnosis is limited because it had been reported that endometriosis had developed after amniosynthesis along the route of the needle 24. Moreover biopsy has been associated to an increased risk of recurrence 13. For this reason, using fine needle aspiration biopsy or core biopsy can be suitable only in the site of future operation. In our case, because operation was planned, to exclude additional pathologies which could change the form of operation core biopsy had been done on the future operation site nearest to the mass.
Accurate diagnosis is reached by histopathology. Endometrial glands and stroma are seen in the histology. In macroscophy, the repeated episodes of bleeding gives rise to severe surrounding fibrosis and scarring 4,5.
Because malign developing in abdominal wall endometriosis, the treatment of choice for endometriosis of the rectus abdominis muscle is a wide local excision of the lesion with negative margins 5,6. Our patient has been subjected to surgery with a wide local excision of the lesion with negative margins. Total wide excision of the lesion is the gold standard for treatment, and it is diagnostic and therapeutic at the same time. Medical treatment with the use of progestogens, oral contraceptive pills, and danazol is not effective, complete regression is rare with medical treatment, gives only partial relief in symptoms 8,16.
In conclusion, scar endometriosis is rare and difficult to diagnose with FM. When a woman presents with a painful swelling in the abdominal scar especially with a history of previous gynecological or obstetrical surgery should have suspicion of scar endometriosis. Endometriosis may occur years after the surgery. Patients with scar endometriosis may be asymptomatic or present with pain.Although the role of methods of imaging is limited in diagnosis, they can help for diagnosis via giving idea about the dimensions, the spread and the relationship with the surrounding tissue of the mass and whether there are concurrent additional pathologies or not. Definitive diagnosis is based on histopathologic analysis. Total wide surgical excision is the gold standard for treatment of abdominal wall endometriosis. Patient should be followed-up for recurrence. Due to the increasing rate of cesarean sections, gynecologic operations, laparoscopies and amniocentesis, an increasing incidence of extrapelvic localization of endometriosis is expected.
References
- Blanco RG, et al. Abdominal wall endometrioma. Am J Surg. 2003;185:596?8.
- Missmer AS, et al. Incidence of laparoscopically confirmed endometriosis by demographic, anthropometric, and lifestyle factors. Am J Epidemiol. 2004; 160;784-96.
- Taff L, Jones S. Cesarean scar endometriosis. A report of two cases. J Reprod Med. 2002;47:50-2.
- Woodward PJ, Sohaey R, Mezzetti TP. Endometriosis: radiologic-pathologic correlation. Radiographics. 2001;21:193?216.
- Coeman V, Sciot R, Van Breuseghem I. Rectus abdominis endometriosis: A report of two cases. Br J Radiol. 2005; 78:68-71.
- Gordon CW, Singh KB. Cesarean scar endometriosis: a review. Obstet Gynecol Surv. 1989;42:89-95.
- Horton JD, Dezee KJ, Ahnfeldt EP, Wagner M. Abdominal wall endometriosis: A surgeon?s perspective and review of 445 cases. Am J Surg. 2008; 196: 207?12.
- Erkan N, Haciyanli M, Sayhan H. Abdominal wall endometriomas. Int J Gynaecol Obstet. 2005; 89: 59?60.
- Douglas C, Rotimi O. Extragenital endometriosis ? a clinicopathological review of a Glasgow hospital experience with case illustrations. J Obstet Gynaecol. 2004;24: 804?8.
- Giannella L, La Marca A, Ternelli G, Menozzi G. Rectus abdominis muscle endometriosis: Case report and review of the literature. J Obstet Gynaecol Res. 2010; 36:902-06.
- Chiang DT, Teh WT. Cutaneous endometriosis-Surgical presentations of a gynaecological condition. Aust Fam Physician. 2006;35:887-8. PMid:17099809.
- Güneş M, Kayıkçıoğlu F, Öztürkoğlu E, Haberal A. Incisional endometriosis after caesarean section, episiotomy and other gynecologic procedures. J Obstet Gynaecol Res. 2005;13:471?5.
- Bumpers HL, Butler KL, Best IM. Endometrioma of the abdominal wall. Am J Obstet Gynecol. 2002;187: 1709-10.
- Singh KK, et al. Presentation of endometriosis togeneral surgeon: a 10 year experience. Br J Surg. 1995;82:1349-51.
|