Abstract
It is very important to determine the etiology of pain in patients presenting to the emergency department with chest pain. Generally, 50% of this chest pain is of cardiac origin, and early diagnosis and treatment can be lifesaving. However, panic disorder accounts for about 30% of chest pain of non-cardiac origin. This necessitates that patients with a diagnosis of panic disorder require a thorough evaluation to eliminate cardiac causes for their symptoms. On coronary angiography, widespread coronary artery disease was diagnosed in a 51-year-old male with a 20-year history of panic disorder who underwent coronary bypass surgery. In this article, we want to emphasize that in patients presenting to a hospital?s emergency department with a history of panic disorder, physicians should exclude cardiac causes for their symptoms.
Keywords :
Panic disorder
, Chest pain
, Acute coronary syndrome
Turkish Abstract
Göğüs ağrısı nedeni ile acil servise başvuran hastaların ağrı nedeninin saptanması çok önemlidir. Bu göğüs ağrılarının %50?si kardiyak kökenli olup erken tanı ve tedavisi hayat kurtarıcıdır. Nonkardiyak göğüs ağrılarının ise %30?luk kısmı panik bozukluk nedeni ile olmaktadır. Acil servise göğüs ağrısı şikayeti ile başvuran ve özellikle de panik bozukluk tanısı olan hastaların ayırıcı tanısı ve tedavisi, ön yargılardan uzak ve olası kardiyak nedenler mutlaka ekarte edilerek yapılmalıdır. Yirmi yıldır panik bozukluk tanısı olan 51 yaşındaki erkek hastaya yapılan koroner anjiyografide yaygın koroner arter hastalığı saptandı ve koroner baypas yapıldı. Bu vaka sunumunda, psikiyatrik hastalarda göğüs ağrısı etiyolojisine azami dikkat edilmesi gerekliliği vurgulanmak istenmiştir.
Turkish Keywords :
, Panik bozukluk
, Göğüs ağrısı
, Akut koroner sendrom
Introduction
Chest pain is one of the most common symptoms directing patients to the emergency department. In approximately half of the cases, chest pain is of either ischemic or non-ischemic cardiac origin. Additionally, research indicates that in 50% of people diagnosed with non-cardiac chest pain, 30% suffer from panic disorder 1. In this article, we want to emphasize that patients admitted to a hospital?s emergency department with panic disorder should be treated carefully while creating a differential diagnosis for chest pain, without pre-judgement, keeping also in mind the possibility of an organic cause.
Case Report
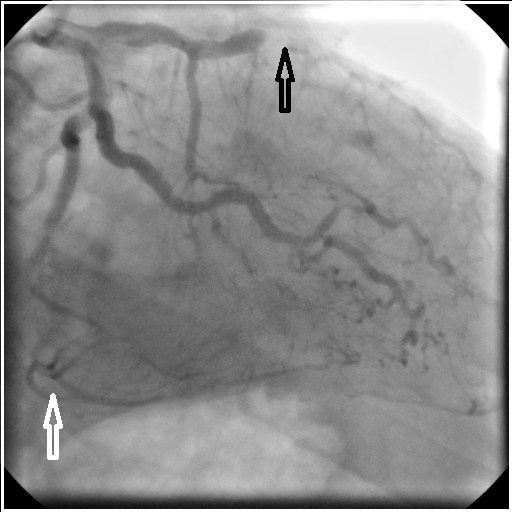
A 51-year-old male with a 20-year history of panic disorder presented to the emergency room with complaints of chest pain, dyspnea, palpitations, dizziness, nausea, and numbness. The patient did not exhibit other physical symptoms or show physical signs with the exception of high triglycerides. During his previous ED visit, his symptoms lasted approximately 15 min and the patient was admistered sedatives and discharged home. During his current visit, the patient was diagnosed with an acute coronary syndrome based on electrocardiography, coronary angiography was performed. Total stenosis of the right coronary artery (RCA) and left anterior descending artery (LAD) was noted (Figure 1) and the patient was scheduled for an urgent coronary artery bypass graft procedure .
On echocardiography, the patient was found to have an ejection fraction of 42% and segmental wall motion dysfunction. Three coronary arteries of the patient were bypassed; LAD-left internal mammary artery (LİMA), RCA- saphenous vein graft, diagonal-saphenous vein graft. The patient had an uneventful post-operative course, and was discharged from the hospital.
Discussion
Acute coronary syndrome (ACS) is a life-threatening condition which benefits from prompt evaluation and proper treatment, such that it would be considered negligent for a physician not to consider it as a possible diagnosis in any patient presenting with acute symptoms of chest tightness or discomfort, palpitations, dyspnea, diaphoresis, nausea and vomiting.
It is particularly important (and difficult) to distinguish chest pain caused by panic disorder and that caused by coronary artery disease (CAD). But are panic disorder and CAD really independent? Currentlypsychiatrists disapprove of mental illness being labeled as?functional?, and physical illness as ?organic?, because of an increasing body of literature that demonstrating a definitive link between mental and physiological processes 2.
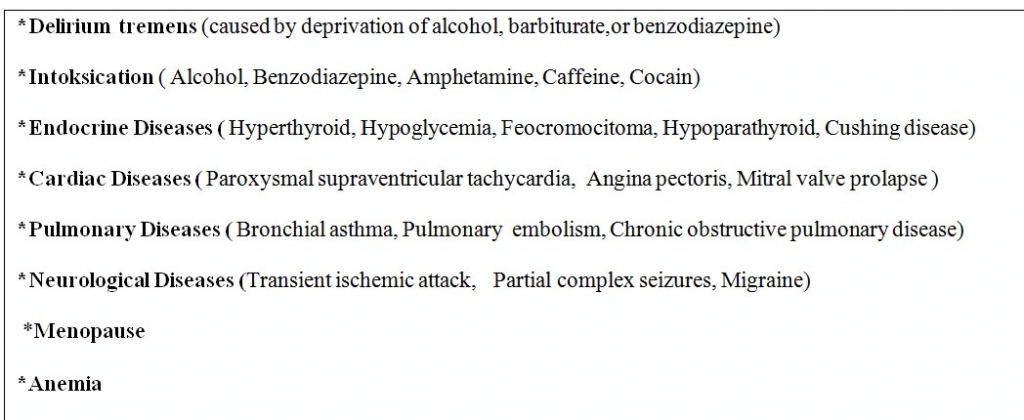
Panic disorder and CAD often coexist, and chest pain in panic disorder may be caused by true CAD. Additionally, panic disorder is common in many organic diseases 3. (Table 1).
Although myocardial ischemia can cause panic attacks via increased catecholamines or by increasing cerebral carbon dioxide levels secondary to lactate, panic disorder is more likely to promote CAD through its relationship with cardiac risk factors. However, the nature of the exact relationship between panic disorder and cardiac risk factors is unclear 4.
Two useful basic investigations in the diagnosis of ACS are the electrocardiogram (ECG) and serum enzyme bio-markers. Dynamic T-wave changes and ST elevation/depression aresome of the features which may be detected on ECG, but it is important to note that an unremarkable ECG does not exclude ACS. Various serum enzymes can serve as biomarkers for myocardial necrosis, with troponin I as the biomarker of choice given its high sensitivity and specificity 2.
In our case, the patient was seen in the emergency department once or twice in a month over the years with panic attacks. However, until his last visit, an accurate investigation for the potential causes of cardiac origin was not carried out. Coronary angiographydemonstratedcomplete occlusion of the right and left coronary artery, and collateral arteries were present indicating that the disease process was not acute with coronary occlusion developing over several years. It is interesting that patients presenting to the emergency room with panic disorder, may, in fact, have a diagnosis of ACS. The most important reason for misdiagnosis is likely the incorrect perception of the disease process formed by patients presenting to the emergency department with complaints of panic disorder.
In conclusion, the cause of chest pain must be accurately diagnosed; and treatment must be pursued based on the etiology of symptoms, especially if the pain is of cardiac origin.
References
- Hamer HP, McCallin AM. Cardiac pain or panic disorder? Managing uncertainty in the emergency department. Nurs Health Sci. 2006 Dec;8(4):224-30.
- Soh KC, Lee C. Panic attack and its correlation with acute coronary syndrome - more than just a diagnosis of exclusion. Ann Acad Med Singapore. 2010 Mar;39(3):197-202.
- R Tükel. Panik Bozukluğu. Klinik Psikiyatri Dergisi, 2002 ; Ek 3: 5-13.
- Katerndahl D. Panic plaques: panic disorder & coronary artery disease in patients with chest pain. J Am Board Fam Pract. 2004 Mar-Apr;17(2):114-26.
|