Abstract
Duodenal webs are rare congenital anomalies which are among the causes of duodenal obstructions. The symptoms and the age of onset may vary depending on the size and location of the duodenal web. Our aim in this case report is to present the radiologic imaging findings of a 6-year old male patient who presented with intermittent vomiting, epigastric distension, fatigue and diarrhea, and was diagnosed with a web in the second portion of the duodenum during exploratory surgery. We also discuss the causes of duodenal obstruction and the related imaging findings in light of the current literature.
Keywords :
Duodenal web
, Duodenal obstruction
, Intermittent vomiting in children
, Windsock deformity
Turkish Abstract
Duodenal web, duodenal obstrüksiyonlar arasında nadir görülen konjenital anomalidir. Duodenal webin büyüklüğü ve yerleşimine göre, bulgular ve başlangıç yaşı değişiklik gösterebilmektedir. Bu olgu sunumunda, tekrarlayan kusma, epigastrik distansiyon, halsizlik, ishal şikayetleriyle başvuran, cerrahi sonucu duodenum ikinci kısmında web saptanan, 6 yaşındaki erkek olgunun radyolojik görüntüleme bulgularını sunmayı, duodenum obstrüksiyon nedenlerini ve görüntüleme bulgularını mevcut literatür bulguları eşliğinde tartışmayı amaçladık.
Turkish Keywords :
, Duodenal web
, Duodenal obstrüksiyon
, Çocukta tekrarlayan kusma
, Windsock deformitesi
Introduction
A duodenal web, which is one of the causes of duodenal obstruction, is a thin, round, partially permeable, web-like structure. It is a rare condition with approximately 100 cases reported in the literature. The web is frequently observed in the second portion of the duodenum 1. The severity of symptoms and the age of onset vary according to the size and location of the web, and if the obstruction is total or partial. Therefore, the diagnosis may be delayed until late childhood or even to adulthood.
Besides duodenal webs, conditions like midgut volvulus, annular pancreas, duplication cysts, superior mesenteric artery syndrome, and periduodenal portal vein are among the reasons for partial obstructions in the duodenum 2. The diagnosis of a partial or total duodenal obstruction can be made based on the clinical and radiological findings. The common findings in these patients are distension in the stomach and duodenum observed in upright abdominal radiograph, air-fluid levels, and normal gas distribution in the more distal intestinal loops. The cause of the partial obstruction may also be diagnosed with the help of additional radiological evaluation methods and endoscopic findings.
Case Report
A six-year old male patient presented with fatigue, vomiting, and diarrhea, which were present for nine months but had recently become more severe. His physical examination revealed epigastric distension. No organomegaly or mass was palpated during the abdominal examination. The patient?s complete blood count and biochemical parameters were within normal limits. He consecutively underwent upright abdominal radiography, upper endoscopy, upper gastrointestinal (GI) gastrogram with small bowel follow-through, and oral + iv contrasted abdominal computed tomography.
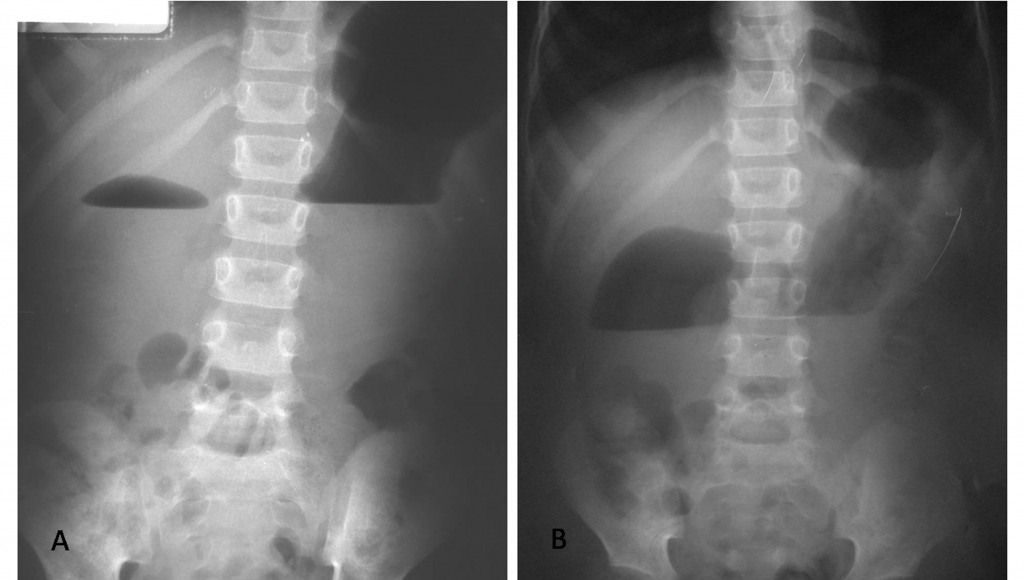
In the upright abdominal radiograph, distension in the stomach and the ??double bubble?? sign were observed. The gas detected within the distal intestinal loops pointed to a partial obstruction (Figure 1).
The ultrasonography revealed a dilated duodenal loop with increased content and reduced motility in the upper right quadrant. The stomach was distinctly distended and its contents were increased. No peristaltic movement was observed during the sonographic examination.
The endoscopy did not indicate any pathological findings other than the distension in the stomach and duodenum. Pathological examination of the biopsies taken from the antrum and duodenum during the endoscopy revealed chronic gastritis, helicobacter pylori infection, normal duodenal villi; and lymphocytes, plasma cells, eosinophils and replete veins among the duodenal glands. Although the endoscopy reached the second portion of the duodenum, no duodenal web was observed.
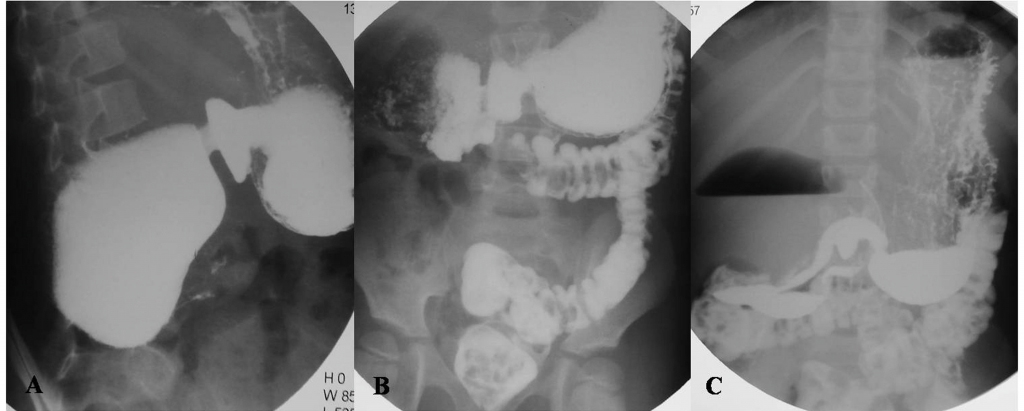
In the esophageal, gastric and duodenal radiography (EGDR), the esophagus was observed to be normal while the stomach and the first and second parts of the duodenum were dilated. Contrast was observed to halt at the distal aspect of the second portion of the duodenum, only to be observed to pass to the distal intestinal loops in the X-rays taken after approximately 15 minutes (Figure2).
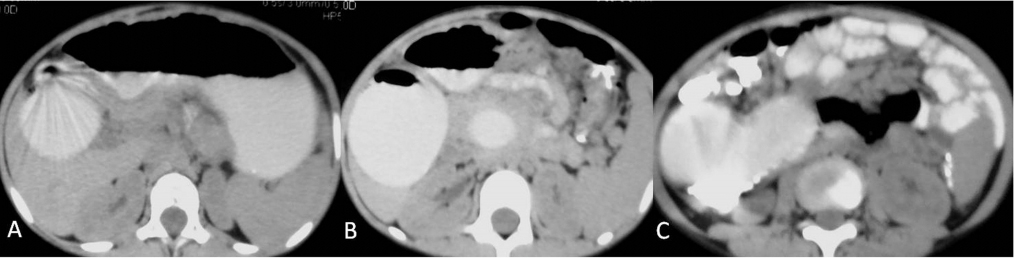
The abdominal computed tomography (CT) noted severe distension in the stomach and in the first and second portions of the duodenum, together with a stenosis in the distal aspect of the second portion. Also, a mild compression of the right kidney was observed due to the duodenal abnormality. The fact that the contrast was noted in the distal intestinal loops despite the stenosis in the second portion of the duodenum pointed to a partial obstruction in that section (Figure 3). However, a specific diagnosis could not be obtained from the tomographic examination.
The patient was taken to surgery with a diagnosis of partial duodenal obstruction, and a web was noted in the distal aspect of the duodenum, which was then excised (Figure 4). Post-operatively, the patient was discharged without any complications, and experienced complete relief from his symptoms on post-surgical follow-up.
Discussion
Stenosis and atresia in the small intestine is a relatively common congenital defect and may occur in any location within the small intestine. The most commonly affected segment is the duodenum, whereas the least affected segment is the ileum. Stenosis and atresia are observed in 2-5 of every 10,000 births 3. Although the diagnosis is made during the neonatal period, depending on the degree of the stenosis, it may be delayed until late childhood or puberty. The clinical presentation of this disease entity includes upper abdominal distension, post-prandial pain, and intermittent emesis secondary to partial or complete duodenal obstruction. However, non-specific abdominal symptoms may also be observed 4. Our patient presented in a similar manner with symptoms of intermittent vomiting and abdominal distension due to a partial obstruction. In pediatric patients, the causes of partial or total duodenal obstruction include duodenal duplication cysts, duodenal web, duodenal atresia, periduodenal portal vein, midgut volvulus, annular pancreas, and superior mesenteric artery syndrome 5.
Duplication cysts are spherical and tubular structures covered by esophageal epithelium and with smooth muscle in their walls. Duplication cysts can occur in any location between the tongue and the anus 6. In contrast to duodenal webs, duplication cysts appear as masses with smooth borders leading to compression of the duodenal lumen on contrast studies. On ultrasonography and CT, the condition is detected as a mass lesion of cystic nature 2.
Annular pancreas is the most commonly observed congenital anomaly of the pancreas where it encircles the second portion of the duodenum, which may lead to an obstruction of the latter 7. Contrast studies point out a concentric stenosis in the involved section with a proximal dilatation as in our patient. The diagnosis is verified through abdominal CT and MRI 8.
Superior mesenteric artery (SMA) syndrome is characterized by a compression of the 3rd portion of the duodenum between the abdominal aorta and the SMA, resulting in expansion of the duodenum and the stomach.
Compression of the 3rd portion of the duodenum due to reasons such as extended bed rest, rapid weight loss, diseases such as pancreatitis or Crohn?s disease that lead to inflammation and fibrosis in the mesenteric root; pancreatic cancer, retroperitoneal masses, scleroderma, etc. lead to temporary obstructions. In our patient, none of these causes or risk-factors were present. Also, the CT did not point out any decrease in the SMA-to-aorta distance or any SMA compression 9.
Duodenal atresia is diagnosed during the intrauterine or neonatal periods. In this condition, usually the 2nd and 3rd portions of the duodenum are involved. In the prenatal US, the fetal abdomen is observed as a double-bubble filled with water. Polyhydramnios and vomiting may be observed. In duodenal atresia, the upright abdominal radiograph does not show any double-bubble sign or abdominal gas in the intestinal loops located more distally from the duodenum. Although the double-bubble was observed in our radiograph, there was abdominal gas also at the distal aspect. Therefore, a partial obstruction was considered 5,10.
Midgut volvulus is most frequently observed within the first week of life. The obstruction occurs when the intestines are suspended by a short mesentery and thus are able to rotate around the SMA axis 11. Since the radiological findings of the volvulus such as the ?corkscrew sign? in the contrast studies and the ?whirl sign? in the abdominal CT were not detected, volvulus was not clinically considered in our patient 12-15.
An intestinal web is a membranous structure within the lumen and consisting of the mucosa, submucosa and the intestinal muscular layer. It is partially permeable at its center 16. During early fetal life, it develops through the incomplete vacuolization and recanalization of the duodenum. The resulting barrier may be complete, or less frequently may have a small orifice which forms a duodenal membrane with fenestration. The continuous peristaltic activity causes the membrane to prolapse distally, forming the wind sock sign 17. This wind sock sign is typical for the duodenal web in contrasted imaging. However, the upper GI series with small bowel follow-through did not reveal this sign in our patient. In cases where the web completely closes the passage, severe vomiting is observed and the disease is diagnosed during the neonatal phase. If, as in our case, the passage is not completely but only partially obstructed, the diagnosis may be delayed until late childhood or even young adulthood. In this case, clinical symptoms like nonspecific abdominal pain primarily in the upper quadrant and the epigastric area, distension, and especially post-prandial vomiting may be observed 1,4,18. Among the cases of duodenal web, 85-90% are located in the second portion of the duodenum, as was the case in our patient 18. Although the upright abdominal radiograph and contrast studies give valuable information for the diagnosis of the web, the actual diagnosis is typically made through endoscopy 4,19. It is claimed that the condition may be viewed using ultrasonography when the duodenum is filled with water; however, the clinical experience of the operator plays a key role in this method 19. In our patient, the imaging studies helped in diagnosing a partial obstruction, although the endoscopy was unable to accurately diagnose the condition. Ultimately it was exploratory surgery with allowed us to diagnose and treat the patient effectively.
In conclusion, duodenal stenosis with partial obstruction may be caused by a web with a small orifice. In pediatric patients where intermittent vomiting, epigastric distension, and duodenal stenosis or obstruction are observed via imaging, duodenal web must also be considered in the differential diagnosis besides other possible diagnoses including duodenal atresia, duodenal duplication cysts, annular pancreas, midgut volvulus, and the SMA syndrome.
References
- Mahajan SK. Duodenal diverticulum: Review of Literature. Indian J Surg 2004; 66: 1450-1453.
- Berrocal T, et al. Congenital anomalies of the upper gastrointestinal tract:RadioGraphics 1999;19: 855-872.
- Lee SS, Hwang ST. A Case of congenital duodenal Web Causing Duodenal Stenosis in a Down Syndrome Child: Endoscopic Resection with an Insulated-Tip Knife. Gut and Liver 2011;5(1): 105-109.
- Melek M, Edirne YE. Two cases of duodenal obstruction due to a congenital web: World J Gastroenterol 2008; 14(8): 1305-1307.
- Auringer RT, Sumner TE. Pediatric upper gastrointestinal Tract. Radiol Clin North Am 1994;32 : 1051-1066.
- Martins JL, et al. Cecal duplications causing a disappearing abdominal mass in an infant. J Pediatr Surg 2001; 36: 1581-1583.
- Yigiter M, et al. Annular Pancreas in Children: A Decade of Experience. EAJM 2010; 42: 116-9.
- Sandrasegaran K, et al. Annular Pancreas in Adults. AJR 2009; 193:455?460.
- Gustafsson L, et al. Diagnosis and treatment of superior mesenteric artery syndrome. Br J Surg 1984; 71:499-501.
- Kocakoç E, Kırış A, Kazez A. Duodenal atresia: Prenatal ultrasonography diagnosis. Diagn İnterv Radiol 2003;111-112.
- Christine MP, et al. Volvulus of the Gastrointestinal Tract: Appearances at Multimodality Imaging.RadioGraphics,2009;29:1281-12931
- Çubuk M, et al. Radiologic findings of midgut volvulus. Diagn İnterv Radiol 2000; 6:227-229.
- Leonidas CJ, et al. Midgut volvulus in infants: diagnosis with US. Radiology 1991; 179:491-493.
- Weinberger E, et al. Sonographic diagnosis of intestinal malrotation in infants: importance of the relative positions of the superior mesenteric vein and artery. AJR Am J Roentgenol 1992; 159:825-828.
- Long FR, et al. Intestinal malrotation in children: tutorial on radiographic diagnosis in difficult cases. Radiology 1996; 198:775-780.
- Jinkins JR, et al. Antral mucosal diaphragms in infants and children. Ped Radiol l980; 9: 69?72.
- Rowe MI, Buckner D, Clatworthy HW Jr. Windsock web of the duodenum. Am J Surg 1968; 116: 444- 449.
- Materne R. The duodenal wind sock sign. Radiology 2001; 218:749-750.
- Yoon CH, et al. Sonographic windsock sign of a duodenal web. Pediatr Radiol 2001; 31: 856-857.
|