Abstract
Basal cell adenoma is a rare salivary gland tumor. These tumors usually occur within the parotid gland, with the submandibular gland being affected in 5% of cases. Fine-needle aspiration cytology provides differentiation between benign and malignant lesions. These tumors arise from epithelial or myoepithelial cells which can be identified by immunohistochemical investigations. This case report describes a basal cell adenoma in the submandibular salivary gland of a 65 year old male, with an emphasis on histopathologic and cytologic features.
Keywords :
Salivary gland tumor
, Basal cell adenoma
, Submandibular gland
Turkish Abstract
Bazal hücreli adenom nadir bir tükürük bezi tümörüdür. Genellikle parotis bezinde görülür. Submandibular bez %5 oranında etkilenir. İnce iğne aspirasyon sitolojisi benign ve malign lezyonları ayırmayı sağlar. Bu tümörler epitelyal ve miyoepitelyal hücrelerden köken alabilir. Kökenleri immunhistokimyasal araştırma ile gösterilir. Bu makalede 65 yaşında erkek hastada submandibular gland yerleşimli bazal hücreli adenom olgusu ve olguya ait histopatolojik ve sitolojik özellikler sunulmuştur.
Turkish Keywords :
, Tükürük bezi tümörü
, Bazal hücreli adenom
, Submandibular bez
Introduction
Salivary gland tumors are uncommon entities that constitute 2 ? 6.5 % of all head and neck tumors 1. Basal cell adenoma (BCA) is a rare benign neoplasm that accounts for 1-3 % of salivary gland tumors. BCA was recognized as an independent entitiy in the second edition of the salivary gland tumors classification of the World Health Organization (WHO) 1,2,3. These tumors affect patients between their fifth and seventh decades with a female predominance. BCA arises most commonly in the parotid gland, although it may also occur in other sites such as the upper lip, buccal mucosa, lower lip, palate and nasal septum 1,2. Fine-needle aspiration cytology (FNAC) is useful in the detection of basaloid neoplasms in well-sampled cases 4. The four sub-types present on histopathologic classification include: solid (monomorphic), trabecular, tubular and membranous 1,2,3. The goal of this study is to describe a basal cell adenoma with cytologic and histopathologic features arising in the submandibular salivary gland, and also to review the literature.
Case Report
A 65 year old male patient was referred to the Otorhinolaryngology Department of the Haseki Training and Research Hospital in 2011 for evaluation of a painless, slow-growing mass in the region around the left submandibular gland. Physical examination revealed a 5 cm well-circumscribed, firm, painless nodule. No inflammation of the overlying skin was noted. No other masses or lymph nodes were observed in the cervical or facial region.
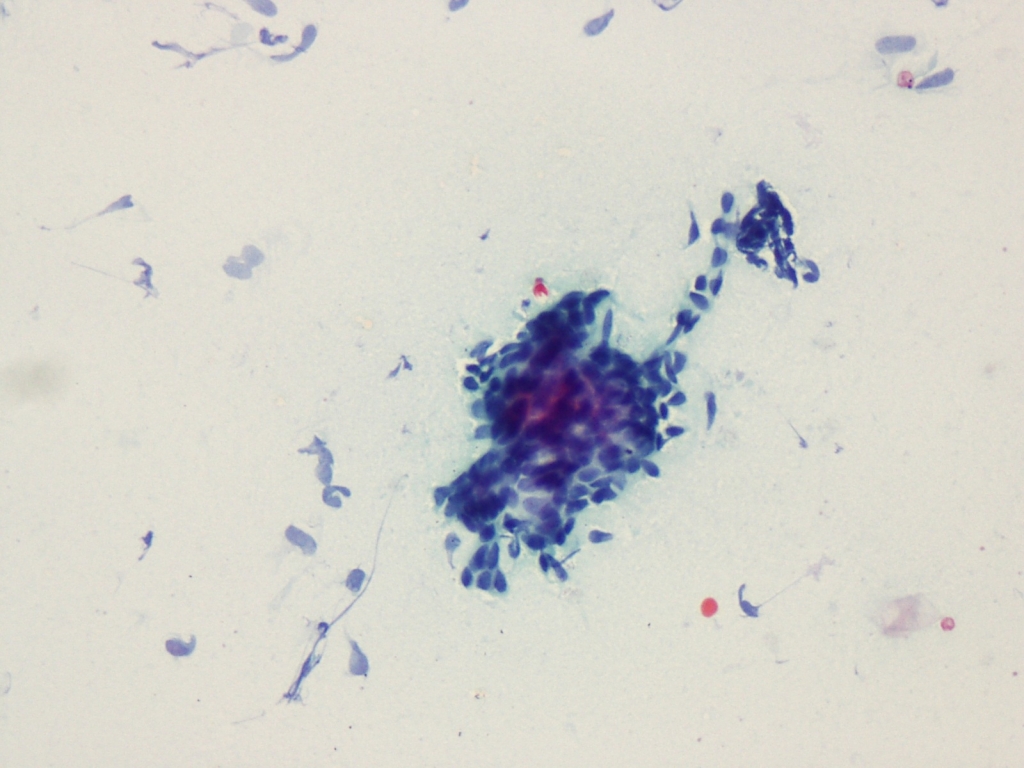
A FNAC was performed and the aspirates were stained with Papanicolaou (PAP) stain. On cytopathologic examination, monomorphic cells with hyperchromatic nuclei, scant cytoplasm and indistinct nucleoli arranged in a solid pattern were observed. No nuclear atypia, mitosis or stromal components were noted (Figure1).
With these findings, the patient was given a diagnosis of monomorphic neoplasia (basal cell adenoma?) and an excisional biopsy was recommended. Subsequently, the patient underwent total excision of the submandibular salivary gland.
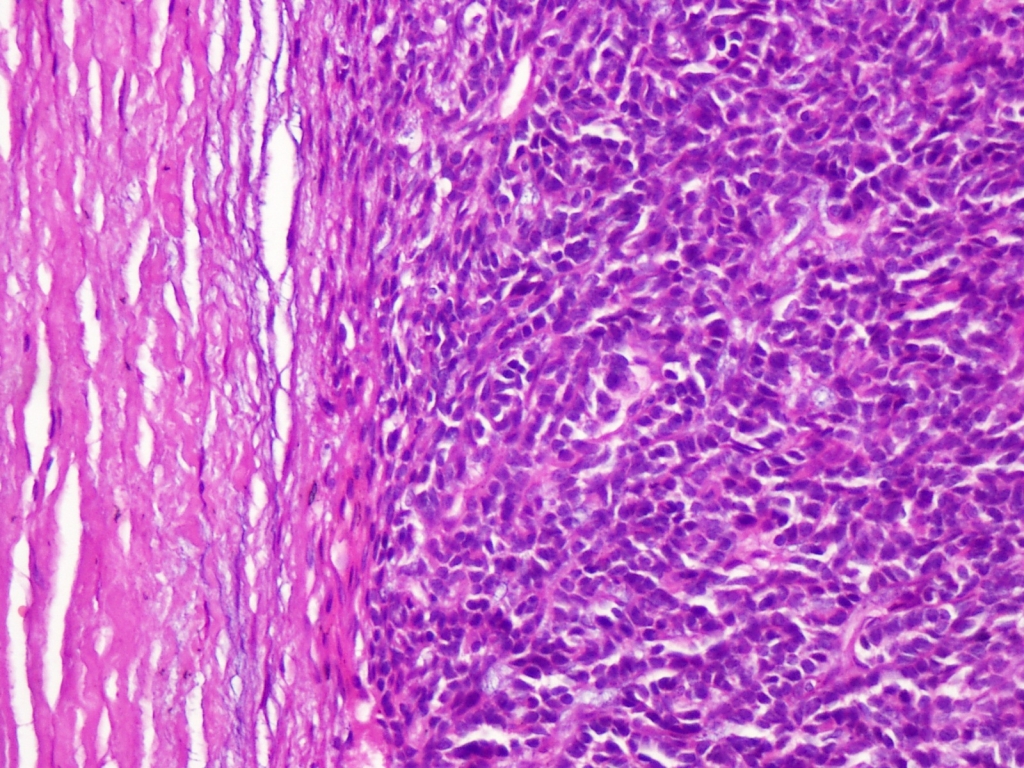
Macroscopic examination revealed an encapsulated, solid, fawn-colored mass measuring 5x4x2.7 cm. The whole tumor capsule was sampled. Histopathologic examination demonstrated small, uniform, dark epithelial cells arranged in a mostly solid but also tubular, trabecular pattern. These cells were noted to be surrounded by fibrous stroma and were enveloped by a fibrous tissue capsule (Figure 2).
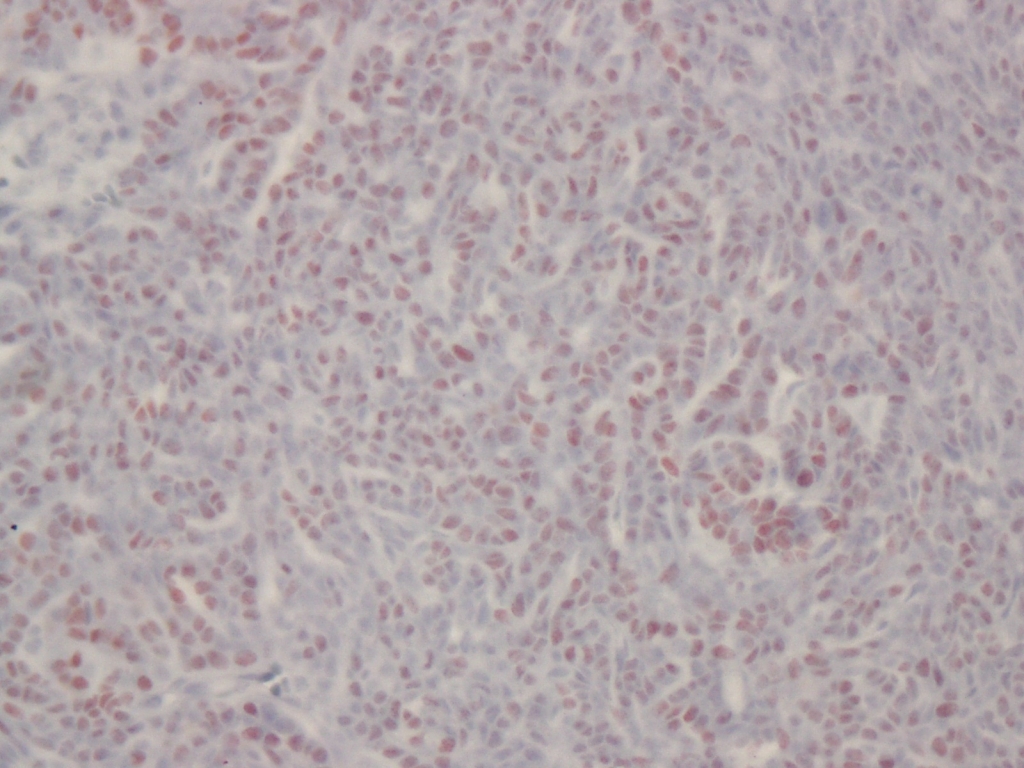
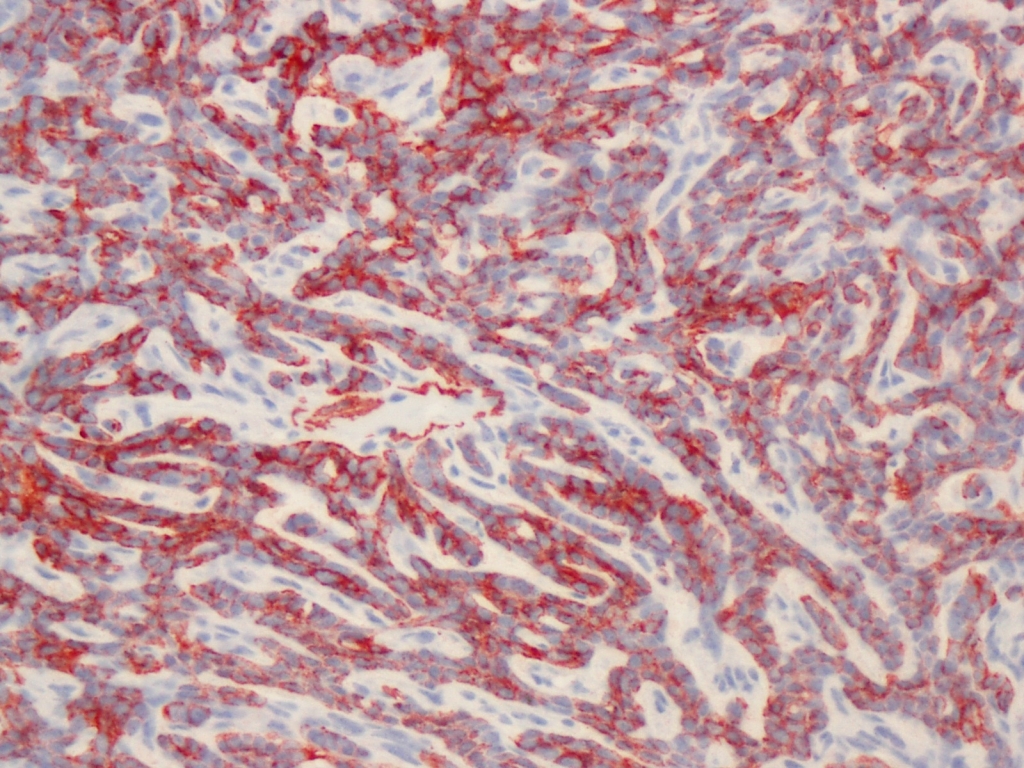
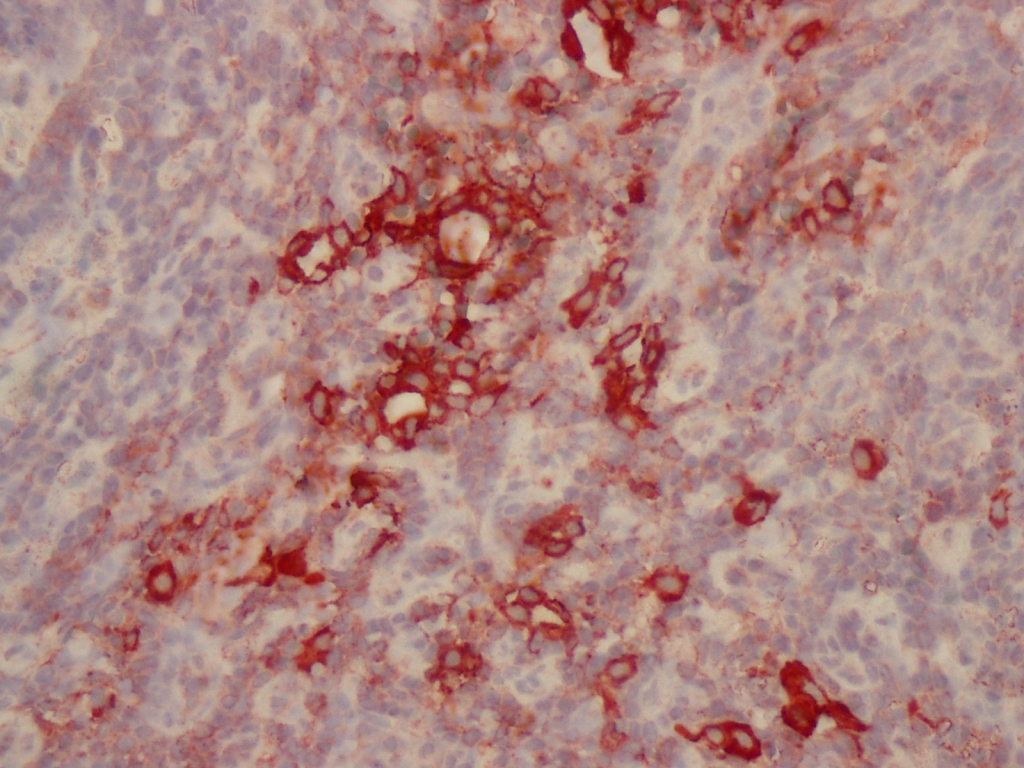
Mitotic rates were rare, and perineural and capsule invasion were not seen. Immunohistochemical investigation showed positive p63, smooth muscle actin (SMA) and immunoreactivity (Figure 3-4).
Cytokeratin7 (CK7) immunoreactivity was seen focally (Figure 5).
Ki-67 proliferation index was less than 5%. Due to these findings, this tumor was diagnosed as a basal cell adenoma.
Discussion
Basal cell adenoma represents 1% to 3% of all salivary gland tumors 1,3,4. It was classified as a subtype of monomorphic adenomas which were first described by Kleinsasser and Klein in 1967 5,6. Currently, basal cell adenomas are classified as subcategories of benign epithelial tumors by the WHO 8. Most of these tumors are located in the parotid gland (75%) and submandibular gland (5%) 5. The minor salivary glands are rarely affected. Gupta et al. described a case of BCA arising in the palatal minor salivary glands 4. Patients with basal cell adenomas are in their 6th-7th decade of life 5. In the literature, gender is controversial with some authors reporting female predominance 1,3,4,5,7 and others reporting male predominance 9. In our case, the basal cell adenoma was located in the submandibular gland of a 65-year-old male patient.
BCAs grow slowly and present as a mobile, firm mass. They are usually asymptomatic. The greatest dimension of these tumors is usually less than 3 cm 2,3. In our case, this tumor was a slow-growing painless mass of 5 cm.
FNAC is highly sensitive in the detection of basaloid neoplasms 4,10. Cytology can be unsatisfactory in cases of BCA with cystic areas 9. Squamous morules are a characteristic feature of basal cell tumors 4. FNAC is performed to distinguish benign lesions from malignant etiologies and aids in the determination of further treatment strategy 10,14. Two populations of epithelial cells are seen; one population has larger nuclei with moderate amounts of cytoplasm, and the other population consists of basaloid cells with dark nuclei, indistinct nucleoli and scant cytoplasm 4,10. Absence of mitosis, necrosis and atypia do not exclude malignancy 10. Cohesive, small basaloid epithelial cells were arranged in a solid pattern in our case. Distinct malignant features, such as mitosis, atypia and necrosis were not observed. For this reason, the tumor was classified as a benign tumor, monomorphic adenoma. In our opinion, aspiration cytology, especially performed with a convenient technique, is useful in the diagnosis of benign lesions. Additionally, the PAP stain provides good nuclecytoplasmic detail.
Histopathologically, BCAs have been classified into solid, trabecular, tubular and membranous types. Cells have a monomorphic, basoloid histologic appearance without a chondromyxoid stroma 2,3,5. The most common type is the solid variant 3. Despite its monomorphic appearance, BCA can stem from more than one cell type such as differentiated ductal cells, poorly differentiated basaloid cells and myoepithelial cells 5,11. Cytokeratin is an immunomarker for epithelial cells while SMA is a marker of myoepithelial cells. These markers show epithelial and glandular origin 12. Nakabayashi et al have demonstrated that the inner cells of the tubular component stain positive for CK7 and negative for SMA. Conversely, the outer cells stain positive for SMA and negative for CK7. BCA is immunreactive for p63, especially at the periphery where tumor cells lie adjacent to the connective stroma 13. In our study similar to the literature, CK7, p63, SMA immunostaining demonstrated the origin and nature of cell types.
Basal cells maybe observed in other salivary gland tumors. In some cases, it may difficult to distinguish between BCA and other primary tumors 1. The basal cell adenocarcinoma, which exhibits a similar imunohistochemical profile, is one of them. It shows an infiltrative growth pattern, perineural or lymphovascular invasion, prominent mitotic activity (more than 4/10HPF), and a high Ki-67 proliferation index (>5%) 2,7. In adenoid cystic carcinomas (ACC), neoplastic cells usually surround the stroma, whereas in BCA, stromal material surrounds neoplastic cells. The matrix material of ACC is transparent and never exhibits squamous differantion 10.
Conclusion
The treatment of BCA is surgical excision 7,9,10. In our case, after one year of post-operative follow up, no recurrence or complication has been detected. FNA allows for the distinction about the benign and malignant nature of tumors and can thus prevent an aggressive surgery. The monomorphic basaloid appearance of cells is very important in the diagnosis of BCA. Tumor cells consist of myoepithelial and epithelial components, which are demonstrated by SMA, p63 and CK7 immunohistochemical markers, despite its monomorphism. Additionally, we wish to highlight the significance of macroscopic examination. The entire capsule must be sampled in order to determine whether an infiltrative growth pattern is present. The pathology report must include the Ki-67 proliferation index and mitotic count, which are required for distinguishing BCA from basal cell adenocarcinomas.
References
- Nakabayashi M, et al. Tubular-trabecular type basal cell adenoma of parotid gland: A patient Report. Yonago Acta medica. 2010; 53:65-9.
- Garcia RG, et al. Basal cell adenoma of the parotid gland. Med Oral Patol Oral Cir Bucal. 2006; 11: E206-9.
- Junquera L, et al. Bilateral parotid basal cell adenoma: An unusual case report and rewiev of the literature. J Oral Maxillofac Surg. 2010; 68: 179-82.
- Gupta N, et al. Basal cell adenoma in a relatively rare site. J Oral Maxillofac Pathol. 2009; 13(2): 101-4.
- Margaritescu CL, et al. Salivary gland basal cell adenomas- immunohistochemical evaluation of four cases and review of the literature. Rom J Morphol Embryol. 2005; 46(1): 29-40.
- Headington JT, et al. Membranous basal cell adenoma of parotid gland, dermal cylındromas, and trichoepitheliomas. Cancer. 1977; 39: 2460-69.
- Esteves ARF, Dıb LL, Carvalho LV. Basal cell adenoma: A case report. J Oral Maxillofac Surg. 1997; 55: 1323-25.
- Barnes L, Eveson JW, Reichart P, Sidransky D (Eds). Tumours of the salivary glands In: World health organization classification of tumours, Pathology and genetics of head and neck tumours.IARC Press: Lyon; 2005. p. 210.
- Gök Ü, Sakallıoğlu Ö, Dağlı AF. Parotis bezinde bazal hücreli adenom: Olgu sunumu. Fırat Tıp dergisi. 2006; 11(2): 150-2.
- Midi A, et al. Basal cell adenoma of salivary gland; cytologic features and differantial diagnosis. KBB- Forum. 2009; 8(4):90- 3.
- Bozdoğan Ö, Atasoy P, Bozdoğan N. Tükrük bezinin bazal hücreli adenomları. Türk Patoloji Derg. 2001; 18(2): 7-10.
- Minicucci EM, et al. Basal cell adenoma of the upper lip from minor salivary gland origin. Eur J Dent. 2008; 2(3): 213-6.
- Edwards P, Bhuiya T, Kelsch RD. Assesment of p63 expression in the salivary gland neoplasms adenoid cystic carcinoma, polymorphous low-grade adenocarcinoma, and basal cell and canalicular adenomas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 97(5): 613-9.
- Satar B, et al. Majör tükrük bezi tümörleri: 93 olgunun analizi. Turkiye Klinikleri JE.N.T. 2001;1(3):123-8.
|