Abstract
Left-sided acute appendicitis is a diagnostic dilemma because of its atypical clinic presentation. Delayed diagnosis is a common feature in this group of patients with left-sided acute appendicitis. We aim to present computed tomography findings of left-sided acute appendicitis with midgut malrotation.
A 63-year-old man presented with 2-day history of loss of appetite and abdominal pain located at left lower quadrant. He was hospitalized with the suspection of diverticulitis clinically. Ultrasonography (US) and Computed Tomography (CT) were performed.
On US a tubular enlarged blind-ending bowel loop arising from cecum, 9 mm in diameter that is was ömnoncompressed with pressure was seen. On CT a right-sided duodenojejunal junction, left positioned cecum and ascending colon were detected. Inverted position of the superior mesenteric vein and artery was also seen. These findings were consistent with midgut malrotation. Dilated appendix with enhancing wall and surrounding fat inflammation was located at the left lower quadrant which was consistent with left-sided acute appendicitis. Although it is a rare cause of left lower quadrant pain, left-sided acute appendicitis should be considered by emergency room physician and radiologists in the differential diagnosis of abdominal pain.
Keywords :
Nonrotation
, Left-sided Acute appendicitis
, Malrotation
Turkish Abstract
Sol taraf yerleşimli akut apandisit atipik klinik bulguları nedeniyle bazen zor tanı alan bir hastalıktır. Bu sunumda orta bağırsak nonrotasyonuna eşlik eden sol yerleşimli akut apandisit olgusunun radyolojik bulgularını sunulmuştur.
Altmış üç yaşında erkek hasta iki gündür devam eden sol alt kadran ağrısı ile hastanemize başvurdu. Daha önce bilinen bir hastalığı olmayan hastanın fizik muayenesinde sol alt kadranda hassasiyet vardı. Lökosit düzeyi 17.500 idi. Hasta akut divertikülit ön tanısı ile hastaneye yatırıldı. Hastaya abdomen ultrasonografi (US) ve bilgisayarlı tomografi (BT) tetkikleri yapıldı.
Abdomen US?de sol alt kadranda komprese olmayan 9 mm çaplı kör sonlanan tübüler yapı saptandı. Sol yerleşimli akut apandisit şüphesi ile yapılan abdomen BT?de çekum ve kolonun bütün diğer segmentlerinin karnın sol yarısında yerleştiği, süperior mezenterik arterin süperior mezenterik venin sağında yerleşim gösterdiği izlendi. Ayrıca sol alt kadranda yerleşim gösteren akut apandisit mevcuttu. Bulgular nonrotasyon anomalisine eşlik eden sol yerleşimli akut apandisit ile uyumluydu. Bu bulgularla opere edilen hastaya appendektomi yapıldı. Postoperatif 3. gün ek sorunu olmayan hasta taburcu edildi.
Sol alt kadran ağrısı ile gelen hastalarda nonrotasyon anomalisine bağlı olarak akut apandisit ayırıcı tanıda akla gelmelidir.
Turkish Keywords :
, Nonrotasyon
, Sol yerleşimli akut apandisit
, Malrotasyon
Introduction
Midgut malrotation is defined as congenital positional anomalies of gastrointestinal tract due to complete or incomplete rotation. The location of intestine segments may vary according to the degree of malrotation. In lack of rotation the cecum localizes at the lower left quadrant of abdomen. In this cases diagnosis of intestinal pathologies such as appendicitis can be difficult. We aim to present computed tomography findings of left-sided acute appendicitis with midgut malrotation.
Case Report
A 63-year-old man presented with 2-day history of loss of appetite and abdominal pain located at left lower quadrant. He had no prior history of significant abdominal pain or any chronic disease. On physical examination he was normotensive (125/75 mmHg), had subfebrile fever (37.1 °C), and localized tenderness at left lower quadrant. There was no abdominal defense.
Complete blood count revealed a white blood cell count (WBC) of 17.500 /mm3.
Abdominal plain X-ray was unremarkable. He was hospitalized with the suspection of diverticulitis clinically. Ultrasonography (US) and Computed Tomography (CT) were performed.
On US (Voluson 730 Pro, GE Healthcare, Milwaukee, WI, USA) a tubular enlarged blind-ending bowel loop arising from cecum, 9 mm in diameter that is was noncompressed with pressure was seen. Contrast enhanced 16-slice multidetector-raw computed Tomography (MDCT) (Brilliance, Philips Medical Systems, Cleveland, Ohio, USA) was performed after US. MDCT images were obtained after injection of 100 mL non-ionic ionidated contrast medium (300mg/dL) at a rate of 3ml/s by a power injector and portal phase images were obtained 80 seconds after intravenous injection. Before the exam oral contrast material (1000mL water and 30 mL Telebrix 35, Guerbet, Cedex, France) was administirated for bowel opacification.
On abdomen MDCT a right-sided duodenojejunal junction, left positioned cecum and ascending colon were detected (Figure 1).
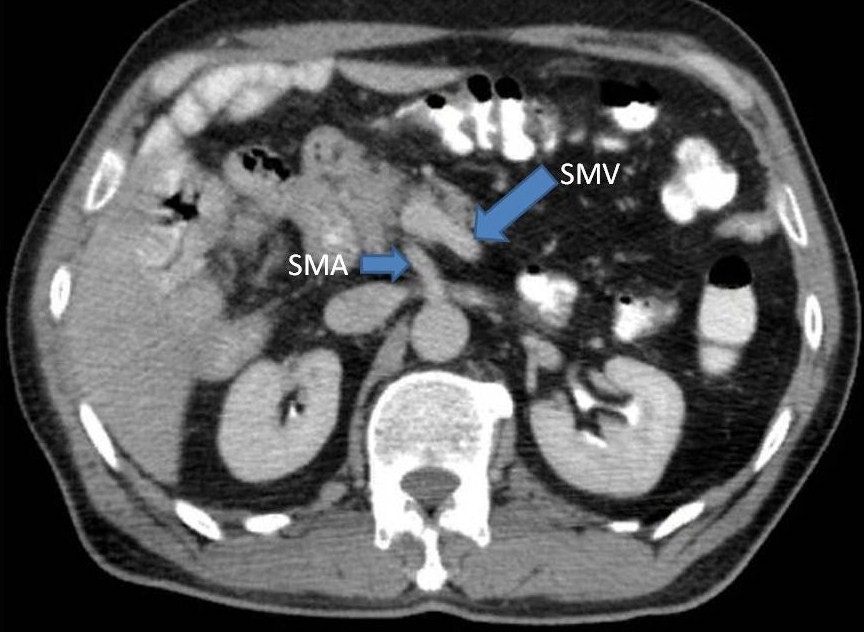
Inverted position of the superior mesenteric vein and artery was also seen (Figure 2).
These findings were consistent with midgut malrotation. Dilated appendix with enhancing wall and surrounding fat inflammation was located at the left lower quadrant which was consistent with left sided acute appendicitis (Figure 3).
Emergency laparotomy was recommended. The patient was taken to surgery and appendectomy was performed through left Mc Burney incision. The diagnosis was confirmed surgically. He was discharged on the third day after surgery without any problem.
Discussion
Many conditions may cause left lower quadrant abdominal pain such as left renal calculi, pyelonephritis, diverticulitis, colitis, inflammatory bowel disease, left ovarian diseases, fibroids, pelvic inflammatory disease 1. Acute appendicitis is a rare cause of left lower quadrant pain. Situs inversus and malrotation of the midgut loop are two anatomic abnormalities that cause left sided appendix 2.
Additionly, inflammation of an extremely long appendix may result left lower quadrant pain. Left-sided appendicitis is difficult to diagnose if there is no previous history about situs inversus or intestinal malrotation.
The embrionic gut is a straight tube at the early stage of development.
During normal midgut rotation a short straight gut rotates 270 counterclockwise around the axis of the superior mesenteric artery between the 4th week and 12th weeks 3.
Errors of rotation that occur at any point during this period results malrotation.
The incidence of intestinal malrotation varies 0.03% to 0.2% depends on kind of study such as autopsy or barium enema studies 4,5. It is difficult to know the true incidence of malrotation in adulthood.
Although midgut rotation anomalies can be symptomatic in childhood, it may have no symptoms untill adulthood. Approximately 60% of cases with malrotation present in the first month of life and 20% present after 1 month in the first year of life 6. Because of its atypical clinic presentation, left sided acute appendicitis is a diagnostic dilemma 7. Delayed diagnosis is a common feature in this group of patients with left-sided acute appendicitis. In elder patients like this case, the clinical manifestation and location of pain can mimic diverticulitis.
Using imaging modalities is essential in the diagnosis of left-sided acute appendicitis.
CT findings of acute appendicitis such as thickening and enhancing of appendix wall, enlargement of appendix, periappendiceal inflammatory changes are well known and CT is an useful and reliable imaging modality in diagnosing acute appendicitis.
CT can diagnose malrotation by the anatomic location of a left sided colon, right sided small bowel, inverted relationship of the superior mesenteric artery and vein 8. Superior mesenteric vein is located at the right side of superior mesenteric artery in normal population, however in the patient with malrotation, superior mesenteric vein is positioned at the left of the superior mesenteric artery 9.
Although it is a rare cause of left lower quadrant pain, left-sided acute appendicitis should be considered by emergency room physician and radiologists in the differential diagnosis of abdominal pain.
References
- Cartwright SL,Knudson MP. Evaluation of acute abdominal pain in adults.Am Fam Physician.2008:1;77(7):971-8.
- Nelson MJ, Pesola GR.Left lower quadrant pain of unusual cause.J Emerg Med. 2001;20(3):241-5.
- Bider K,Kaim A,Wiesner W,Bongartz G. Acute appendicitis in a young adult with midgut malrotation: a case report.Eur Radiol.2001;11(7):1171-4.
- Malek MM,Burd RS. Surgical treatment of malrotation after infancy: a population-based study.J Pediatr Surg.2005;40(1):285-9.
- Forrester MB,Merz RD. Epidemiology of intestinal malrotation, Hawaii, 1986-99.Paediatr Perinat Epidemiol.2003;17(2):195-200.
- Welte FJ, Grosso M.Left-sided appendicitis in a patient with congenital gastrointestinal malrotation: a case report.J Med Case Reports. 2007: 19;1:92.
- Akbulut S, Caliskan A, Ekin A, Yagmur Y. Left-sided acute appendicitis with situs inversus totalis: review of 63 published cases and report of two cases.J Gastrointest Surg. 2010;14(9):1422-8. Epub 2010 Jun 22.
- Zissin R, Rathaus V, Oscadchy A, Kots E, Gayer G, Shapiro-Feinberg M. Intestinal malrotation as an incidental finding on CT in adults.Abdom Imaging. 1999;24(6):550-5.
- Nichols DM, Li DK.Superior mesenteric vein rotation: a CT sign of midgut malrotation.AJR Am J Roentgenol. 1983;141(4):707-8.
Information Presentation
Ulusal Radyoloji kongresi 2011 poster bildiri
|