Abstract
Foramen Winslow herniation is an infrequent herniation type among internal hernias. Clinical signs can be various ranging from minimal digestive disorders to the acute abdomen.
A sixty-eight-year-old female patient was applied to the Emergency Department with abdominal pain which started almost a week ago. She was diagnosed with intestinal perforation after clinical evaluation,and emergancy surgery was planned. Hepatic flexure and the distal part of the ascending colon were observed herniated under the hepatoduodenal ligament through the foramen Winslow, and ischemic, and perforated at the exploration.
Due to the absence of typical clinical findings, and the rarity of this entity, it might be not easy to diagnose the Foramen of Winslow herniation. Delayed diagnosis may result in herniated bowel loops tissue ischemia, and even perforation. There is not any consensus for treatment modality for foramen Winslow herniation. The decision on the treatment could be considered during the operation.
Keywords :
foramen of Winslow
, internal herniation
, perforation of colon
Turkish Abstract
Foramen Winslow hernisi internal herniler arasında nadir görülen bir herniasyon türüdür. Klinik belirtiler minimal sindirim bozukluklarından akut karına kadar değişkenlik gösterebilrir.
Altmış sekiz yaşında kadın hasta, yaklaşık bir hafta önce başlayan karın ağrısı şikayetiyle acil servise başvurdu. Klinik değerlendirme sonrasında bağırsak perforasyonu tanısı konan hastaya acil ameliyat planlandı. Eksplorasyonda hepatik fleksura ve çıkan kolonun distal kısmının hepatoduodenal ligaman altından foramen Winslowdan herniye olduğu, iskemik olduğu ve perfore olduğu gözlendi.
Tipik klinik bulguların olmaması ve nadir görülmesi nedeniyle Foramen of Winslow herniasyonunun teşhis edilmesi kolay olmayabilir. Gecikmiş tanı bağırsak herniye dokunun iskemisine ve hatta perforasyona neden olabilir. Foramen Winslow herniasyonunun tedavi yöntemi konusunda fikir birliği yoktur. Tedavi kararı operasyon sırasında verilebilir.
Turkish Keywords :
, foramen of Winslow
, internal herniasyon
, colon perforasyonu
Introduction
Abdominal hernias have two main groups: internal hernias and external hernias. External hernias are defined as protrusion of abdominal tissues through a defect on the abdominal wall 1. Internal hernia can be defined as a protrusion of the abdominal viscus through a peritoneal and/or mesenteric aperture into the abdominal and pelvic cavity as well 2–4. This aperture can be congenital or acquired secondary to surgery, trauma, or inflammation. Congenital apertures can be a normal orifice such as the foramen of Winslow or can be caused by abnormal intestinal rotation and peritoneal attachments 1,3. The incidence of internal hernias is not related to age or sexuality 2. Clinical signs can be various ranging from minimal mild digestive disorders to the acute abdomen according to the width of the hernia’s aperture, length and, motility of herniated intestinal loops, and presence or absence of strangulation or incarceration 3. Welch describes the classification of internal hernias according to the anatomical location of the orifice where intestinal loops herniate. Paraduodenal hernia (right or left) is the most frequently diagnosed internal hernia subtype with an incidence rate of 53%. The other types of internal hernias were described as pericecal hernias (13%), foramen of Winslow hernias (8%), transmesenteric hernias (8%), intersigmoid hernias (6%), supravesical and pelvic hernias (6%), and trans-omental hernias (1-4%) 5. Even though para-duodenal hernias are known as the most commonly diagnosed internal hernia type, the incidence of trans-mesenteric hernias is increasing due to the increased frequency of gastric bypass surgeries recently 3,4. Foramen of Winslow is a physiological formation which is located beneath the free edge of the lesser omentum and hepatoduodenal ligament, superior to the second portion of the duodenum, and anterior to the inferior vena cava, and provides a connection between the greater and lesser peritoneal cavities 3. Small bowel loops are most commonly herniated viscus with a rate of 60-70%, in foramen of Winslow hernia cases. Rarely, the cecum, ascending colon, gallbladder, transverse colon, and omentum are reported as herniated organs from the foramen of Winslow 1,3. The long mesentery of the small bowel and enlarged foramen of Winslow are the most commonly reported risk factors for this clinical situation 6. Patients generally present with acute and progressive abdominal pain with accompanying small bowel obstruction signs like nausea and vomiting as a result of compression on the stomach by herniated tissue 1,7. Computed Tomography (CT) is frequently required to diagnose an internal hernia. An image of an obstructed intestinal loop, trapped between hepatic hilum and stomach and pancreas on a CT scan can be helpful for diagnosis 5,6. Obstructive jaundice secondary to compression of the cholecodh duct which is placed in the hepatic pedicle by herniated tissue can be observed as well 3.
Case Report
A 68-year-old female patient was admitted to the emergency department with acute abdomen clinical signs. Her complaints started with mild abdominal pain and distension almost a week ago. Her complaints worsened in a few days, and fever, nausea, and vomiting were added to her clinic. Abdominal distension and peritonitis signs like defense and rebound signs were detected to be positive at her physical examination. Infection parameters like C-Reactive Protein (CRP:11.7 mg/dL), Procalcitonin (5.7 ng/mL), White Blood Cells (WBC:11.7 10³/uL), and liver enzymes like Aspartate Aminotransferase (AST:191 U/L) and Alanine Aminotransferase (ALT: 149 U/L) were detected elevated at the blood tests of the patient. Free air in the abdominal cavity and dilated colonic segment images on the right superior side of the abdomen were observed on the CT scan (Figure 1).
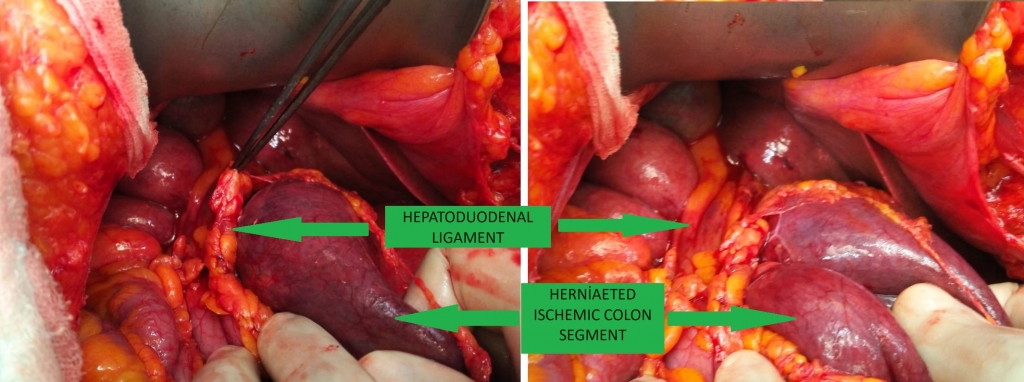
Therefore, surgical exploration was considered with a preliminary diagnosis of intestinal perforation. Chronic diseases such as Diabetes Mellitus (DM), hypertension (HT), and Chronic Obstructive Pulmonary Disease (COPD) were identified in her medical history and there was no other surgical history. She was started on intravenous Seftriakson and Metronidazol as ampiric treatment was started before the operation. After the laparotomy, hepatic flexure and the distal part of the ascending colon were observed herniated under the hepatoduodenal ligament through the foramen of Winslow (Figure 2).
The herniated part of the colon wall was observed as ischemic and perforation was detected on the posterior wall of the ischemic colon. Therefore, the right hemicolectomy and ileo-transverse anastomosis procedure were decided. The right colon was dissected from the right lateral wall, and the mesentery of the right colon was dissected after vascular supplies were ligated, and the right hemicolectomy was performed properly. The side-to-side anastomosis was carried out between the terminal ileum and transverse colon using an 80-mm-linear stapler. Performing a loop ileostomy was thought to be a better choice considering the patient's comorbidities and clinical situation, and the infection of the abdominal cavity secondary to intestinal perforation. The patient was taken to the Intensive Care Unit (ICU) after the surgical procedure was completed. Oral feeding was started on the postoperative 1st day. She was discharged in good condition on the postoperative 7th day with no complications.
Discussion
Internal hernias are the rare cause of intestinal obstructions with a rate of 0.5-4 %. Foramen of Winslow hernias are an infrequent subtype of internal hernias and about 200 cases have been reported in the literature 8. The foramen of Winslow remains closed under normal circumstances. However, if this aperture enlarges enough or abnormally long small bowel loops force the foramen, then intestinal herniation may occur 6,9. Other rare risk factors for this hernia include the persistence of the ascending mesocolon allowing for an excessively mobile bowel, an elongated right hepatic lobe which is thought as a reason mobile intestinal loops pass through the foramen of Winslow, history of cholecystectomy, a "wandering cecum," and defects of the gastro-hepatic ligaments 10. Clinical signs may present with acute and progressive abdominal pain with accompanying small bowel obstruction signs due to compression on the stomach by herniated tissue 1,7,8. Cross-sectional imaging with intravenous contrast-enhanced CT of the abdomen and pelvis is the gold-standard diagnostic imaging modality for internal herniation 9. An obstructed intestinal loop image, trapped between the hepatic hilum and stomach and pancreas on a CT scan might be helpful for diagnosis 5,6. Obstructive jaundice associated with compression of the hepatic pedicle by herniated tissue can be observed, as well 3. Pernice et al, mentioned that narrowing of the portal vein on abdominal CT is another characteristic finding for foramen of Winslow hernias 10. Elevated liver function tests are another result of the compression of the hepatic pedicle as in our case. Even through the radiological imagining, foramen of Winslow hernias can only be diagnosed at a rate of 10% before the operation 11. Therefore, surgical intervention is mandatory to diagnose the exact pathology and perform the treatment. Delayed diagnosis may result in ischemia or perforation of the herniated bowel loops which has high mortality and morbidity rates 10,12. There is no consensus for treatment modality for foramen of Winslow hernias. In case of herniation of hepatic flexure and right colon, right hemicolectomy is the preferred option for treatment to avoid recurrence. Some cases were reported with only fixation of the cecum or right colon or hepatic flexure to avoid recurrence of hernias. In case of incarceration that prevents reduction, decompression by a needle or appendectomy might be required 13. Additional procedures like loop ileostomy might be required according to the clinical situation of the patient, as we performed on our patient. Moris et al. reported no postoperative complications were observed in the comparison of the two groups with and without performing obliteration of the foramen of Winslow during the surgery (10). Nevertheless, surgical closure of the foramen of Winslow is not generally suggested because of the injury risk of the portal vein or choledochal duct, and a beneficial result is not reported to avoid the recurrence of herniation 9,14. Laparotomy is generally the preferred method for the operation instead of laparoscopy, to prevent an iatrogenic intestinal injury of dilated bowel loops secondary to intestinal obstruction clinic. However, in some selected cases, if a definitive diagnosis was made, laparoscopy can be a choice depending on the surgeon’s decision and experience and the patient's clinical situation (9). According to a literature review made by Ayoob et al., the laparoscopic approach has been reported with a rate of 25% 15.
Conclusion
The Foramen of Winslow hernias remains difficult to diagnose due to its rarity and non-specific presentation. There is no agreed global management modality for this clinic. But we emphasize the importance of the early diagnosis to avoid strangulation or perforation which may result in life-threatening clinical situations. Also, this may need organ and tissue extraction like right hemicolectomy or additional surgical inventions and morbidities like loop ileostomy.
Informed Consent
Hastanın kendisinden
References
- Martin LC, Merkle EM, Thompson WM. Review of Internal Hernias: Radiographic and Clinical Findings. Am J Roentgenol. 2006;186:703–17.
- Akyildiz H, Artis T, Sozuer E, Akcan A, Kucuk C, Sensoy E, et al. Internal hernia: Complex diagnostic and therapeutic problem. Int J Surg. 2009 Jan 1;7(4):334–7.
- Lanzetta MM, Masserelli A, Addeo G, Cozzi D, Maggialetti N, Danti G, et al. Internal hernias: a difficult diagnostic challenge. Review of CT signs and clinical findings. Acta Bio Medica Atenei Parm [Internet]. 2019 [cited 2022 Mar 13];90(Suppl 5):20. Available from: /pmc/articles/PMC6625567/
- Wilkes J, Cullen JJ. Internal Hernias: Congenital and Acquired. Shackelford’s Surg Aliment Tract, 2 Vol Set [Internet]. 2019 Jan 1 [cited 2022 Mar 13];858–63. Available from: https://linkinghub.elsevier.com/retrieve/pii/B9780323402323000741
- Murali Appavoo Reddy UD, Dev B, Santosham R. Internal Hernias: Surgeons Dilemma-Unravelled by Imaging. Indian J Surg [Internet]. 2014 Aug 1 [cited 2022 Mar 13];76(4):323–8. Available from: https://link.springer.com/article/10.1007/s12262-012-0620-7
- Mathieu D, Luciani A. Internal Abdominal Herniations. http://dx.doi.org/102214/ajr18321830397. 2012 Nov 23;183(2):397–404.
- Leung E, Bramhall S, Kumar P, Mourad M, Ahmed A. Internal Herniation Through Foramen of Winslow: A Diagnosis Not to Be Missed. Clin Med Insights Gastroenterol [Internet]. 2016 Jun 12 [cited 2022 Mar 13];9:31–3. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27330337
- Abu-Swis S, Cohen N, Wallach N, Abo-Sharb A, Sebbag G, Kian W. Foramen of Winslow hernia years after a Ladd’s procedure: A case report. Int J Surg Case Rep. 2020 Jan 1;72:556–9.
- Mulkey E, Stewart G, Enrique E, El-Sabrout R. A Case Report of a Cecal Bascule with Internal Herniation through the Foramen of Winslow. Authorea Prepr [Internet]. 2021 Oct 20 [cited 2022 Feb 20]; Available from: https://www.authorea.com/doi/full/10.22541/au.163473615.59863148?commit=077db57863cf31f09cd99ac49e986ccf76be1095
- Moris D, Tsilimigras DI, Yerokun B, Seymour KA, Guerron AD, Fong PA, et al. Foramen of Winslow Hernia: a Review of the Literature Highlighting the Role of Laparoscopy. J Gastrointest Surg [Internet]. 2019 Oct 1 [cited 2022 Feb 20];23(10):2093–9. Available from: https://link.springer.com/article/10.1007/s11605-019-04353-3
- Downs P, Downes N, Zayshlyy E, Esper C, Giuseppucci P. Internal hernia through the foramen of Winslow. J Surg Case Reports [Internet]. 2018 Dec 1 [cited 2022 Mar 14];2018(12):1–3. Available from: https://academic.oup.com/jscr/article/2018/12/rjy329/5238825
- Buisset C, Postillon A, Aziz S, Bilbault F, Hoch G, Nesseler J-P, et al. Laparoscopic management of an ascending colon hernia through the foramen of Winslow. J Surg Case Reports [Internet]. 2020 Sep 1 [cited 2022 Feb 20];2020(9):1–3. Available from: https://academic.oup.com/jscr/article/2020/9/rjaa283/5902512
- Jansen YJL, Nieboer K, Senesael E, Van Bael K, Allaeys M. Internal herniation through the foramen of Winslow: a case report. https://doi.org/101080/0001545820181515396 [Internet]. 2018 Mar 3 [cited 2022 Feb 20];120(2):136–8. Available from: https://www.tandfonline.com/doi/abs/10.1080/00015458.2018.1515396
- Fujihata S, Kitagami H, Yamamoto M, Nonoyama K, Suzuki A, Tanaka M, et al. A post operative complication of foramen of Winslow hernia with left to right herniation of the small intestine: An extremely rare case report. Int J Surg Case Rep. 2018 Jan 1;49:219–22.
- Ayoob F, Michael R, Chadnick Z, Fasanya C. Internal hernia of caecum through the foramen of Winslow. BMJ Case Reports CP [Internet]. 2019 Jul 1 [cited 2022 Feb 20];12(7):e228239. Available from: https://casereports.bmj.com/content/12/7/e228239
Information Presentation
This study was presented at the 13th International Hippocrates Congress on Medical and Health Sciences Congress as an oral presentation.
|