Abstract
It is currently known that metastatic breast cancer (BC) has a poor prognosis. The patients usually undergo palliative surgical procedures and are treated symptomatically. Even if the current guidelines do not recommend surgery in the treatment of abdominal metastases derived from breast cancer, some centers suggest surgical treatment, especially in patients with solitary metastases. Here, we described a unique case of a recurrent breast cancer patient with peritoneal carcinomatosis and irresectable big mass in the right lower quadrant of the abdomen who had complete remission after systemic treatment.
Keywords :
Metastatic breast cancer
, abdominal metastasis
, debulking surgery
, chemotherapy
, immunotherapy
Turkish Abstract
Metastatik meme kanserinin prognozu günümüzde halen kötü seyretmektedir. Hastalar genellikle palyatif cerrahi işlemlere tabi tutulmakta ve semptomatik olarak tedavi edilmektedir. Meme kanserinden kaynaklanan abdominal metastazların tedavisinde güncel kılavuzlar cerrahiyi önermese de bazı merkezler özellikle soliter metastazlı hastalarda cerrahi tedaviyi önermektedir. Burada, karın sağ alt kadranda irrezektabl büyük kitlesi ve peritoneal karsinomatozisi olan, sistemik tedavi sonrası tam remisyona giren, nüks meme kanserli nadir görülen bir vakayı inceledik.
Turkish Keywords :
, Metastatik meme kanseri
, abdominal metastaz
, debulking cerrahi
, kemoterapi
, immunoterapi
Introduction
Metastatic breast cancer (BC) has a very poor prognosis, given the lack of reliable curative medical or surgical approaches. Stage IV BC patients usually undergo palliative surgical procedures and symptomatic treatment. Since bone, lung and liver are the most common metastatic sites, peritoneal metastasis (PM) from BC is a rare (3-6%) and challenging clinical picture. These patients with PM were shown to have lower survival rates than those patients with other distant organ metastases. The prognosis for patients with PM is usually short (7-26 months). Currently, there is a lack of evidence and specific recommendations for the management of PM in BC patients 1,2,3.
Below we present a patient with originally triple-negative invasive BC in which the metastatic intraabdominal mass and PC were almost completely remitted after palliative resection and adjuvant systemic therapy.
Case Report
The patient was 54 years old lady with a BMI of 31. In February 2018, she was admitted with a mass in her left breast. On physical examination, an irregularly circumscribed, firm mass of approximately 4x3 cm was palpated at the 12 o'clock position of the left breast. The mammogram showed limited unclear heterogeneous opacity in the upper left quadrant and it was assessed as BI-RADS 4. On ultrasound (US), an irregular hypoechoic solid lesion measuring 17x11 mm was detected at a distance of 3 cm from the areola at a level of 12 o'clock on the left breast, and a core biopsy was taken from this lesion. There were no abnormal enlarged lymph nodes in both axillae. Core biopsy revealed invasive ductal carcinoma and both estrogen and progesterone receptor expressions were 0%, as well as cerb-B2 expression was zero (no staining) on immunohistochemistry (IHC) staining. There was no information about Ki-67 expression. Bilateral breast MRI examination revealed an irregularly shaped, type 2-style contrast-enhanced mass with a diameter of 2.5 cm at 12 o'clock in the left breast, predominantly peripheral, partially central contrast-enhanced. These findings suggested multicentric BC. PET-CT also revealed an intense hypermetabolic lesion of a malignant character (SUVmax: 8.9) at 12 o'clock in left breast.
The patient had a history of heart valve thickening, panic disorder, and herniated disc and previously underwent appendectomy and hemorrhoidectomy. She had been using sertraline as an antidepressant. There was no family history indicating hereditary BC.
As the surgical treatment, the patient underwent a left simple mastectomy and sentinel lymph node biopsy (SLNB) in April 2018. The pathology report revealed 3 cm unifocal invasive carcinoma (NST) and 3 tumor-free sentinel lymph nodes. The tumor was staged as pT2N0 (AJCC, 2018). Histological grade (Nottingham) was III. All margins were cancer-free. No lymphovascular and perineural invasions were reported. IHC studies revealed ER 0 %, PR 0 %, cerb-B2 negative (0/+++) and Ki-67 50 %. Also, p63, CK5/6, CD10 and CK7 expressions were negative.
After the surgery, she received 4 courses of epirubicin and cyclophosphamide, and 12 courses of paclitaxel. She did not receive adjuvant radiotherapy.
Since the patient’s gene tests revealed a pathogenic mutation in BRCA1 gene, the patient was offered risk-reducing right mastectomy and bilateral salpingo-oophorectomy. She underwent only bilateral salpingo-oophorectomy with total abdominal hysterectomy in November 2018. According to the pathological examination report, intramural fibroids with a size of 1.5x1x1 cm were reported as leiomyoma in the endometrial cavity. Endometrium was atrophic, nabothian cysts were present in the cervix, and bilateral ovaries and tubes were normal.
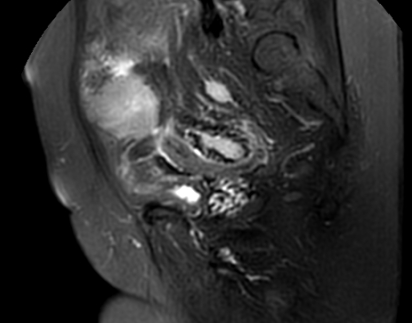
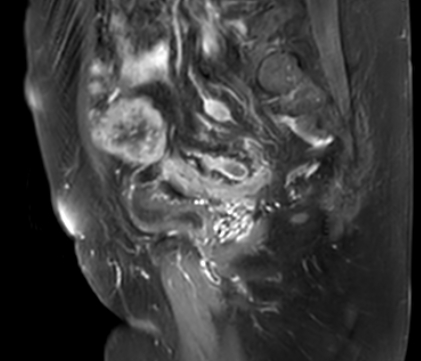
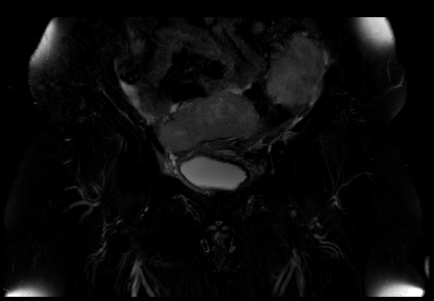
In the follow-up, the patient was admitted to the general surgery outpatient clinic on September 2021 with complaints of increasing abdominal pain which was apparent for the last 3 months. On physical examination, a palpable mass and tenderness were present in the abdomen. Mass formations were found at abdominal US imaging. Abdominopelvic CT showed massive lesions at the pelvic level and in the midline with soft tissue density, the largest of which was approximately 70x40 mm in size. In abdominal contrast-enhanced MRI examination, heterogeneous contrasted mass lesions were observed in the pelvic region, the largest being 10 cm-size, and revealed diffusion restriction on the omental surfaces. The appearance of a free fluid reaching a thickness of 2,5 cm was observed in the abdomen. The anus, perianal regions, and other pelvic intestinal formations were evaluated within normal limits (Figures 1,2,3).
At the colonoscopic examination, there were no pathological findings in the colon and rectum mucosa examined up to 30 cm that could be reached. No pathological findings were detected in the anorectal examination.
The patient was taken to abdominal exploration. During the operation, a tumoral mass originating from the omentum and extending to the pelvis, especially to the right side, was observed. Carcinomatosis appearance was observed on peritoneal surfaces. A large amount of ascites fluid was present. The mass beginning from the omentum was extending to the pelvis. Especially in the right iliac fossa, the mass was fixed and it was extending to the bladder, right ureter and iliac vascular structures. The tumor could be partially resected and therefore residual tumor in the pelvic region was left behind.
Pathological assessment for resected specimens intertwined with omental tissue revealed that the tumoral lesions are metastasis of poorly differentiated carcinoma in adipose tissue. It was interpreted in favor of BC metastasis and abdominal ascites fluid cytologically revealed tumor cells as positive for malignancy. IHC studies revealed that GATA3 negative, mammaglobin negative, PR 0%, ER moderately positive in 50% of neoplastic cells and c-erbB2 negative (0/+++).
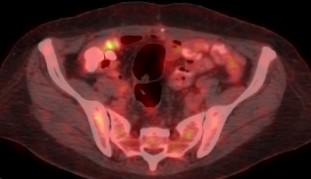
In the F18 FDG PET/CT study taken in the follow-up after surgery, malignant hypermetabolic thickening/soft tissue density lesions on peritoneal mesenteric omental fatty plans and serosal surfaces were reported. The most pronounced at the perihepatic distance were malignant hypermetabolic hypodense lesions, at the level of segments 6 and 7. Hypermetabolic lymph nodes can be classified as malignant at number 7 and 9R levels in mediastinal, anterior diaphragmatic, celiac, paraesophageal, paraaortocaval and bilateral iliac lymphatic stations. At the bilateral parasternal distance, at the lymphatic station number 3A in the mediastinum, slightly hypermetabolic at the paracardiac distance, lymph nodes were limited to centimeters in size. Bilateral pleural effusion, more prominent on the left and free fluid in the abdomen and pelvis was reported.
After the surgery, the patient received palbociclib + letrozole treatment for 3 months. Due to recurrent ascites and the need for paracentesis, this treatment was stopped and chemotherapy (CTX) was planned. She received 15 course of carboplatin and 18 course of paclitaxel. Carboplatin was stopped due to severe nausea, sweating, itching, and dyspnea.
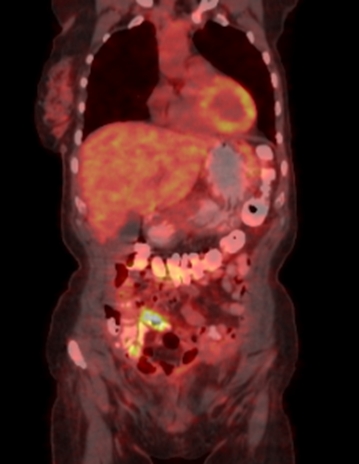
After this treatment, the latest PET-CT, done in May 2022, showed findings consistent with tumor regression. Minimal free fluid was observed in the abdomen and pelvis, and a decrease in its amount was noted compared to the previous study. Lymph nodes showing intense FDG involvement monitored in both parasternal areas, lymphatic station number 3A in the mediastinum and paracardiac distance that were seen in previous FDG PET/CT examination showed significant anatomical /metabolic regression in the current study. No pathological FDG involvement was detected in the millimetric lymph node monitored in the right parasternal area. No characteristic lesion/lymph node showing abnormal FDG uptake was observed in the operation cavity, right breast and both axillary areas similar to the previous study. In a 6 mm nodular lesion observed in the apicoposterior segment of the upper lobe of the left lung, FDG involvement of a pathological uptake was not detected similar to the previous study. The pleural effusion in both hemithorax that was observed in the previous study was not evident in the current one. Lymph nodes showing an intense level of FDG uptake in the mediastinum at lymphatic stations number 7 and 9R in the previous study were not evident in the current one as well. (Figures 4 and 5)
The patient was still on CTX when this report was written.
Discussion
Here in this report, we described a unique case of a BC patient who relapsed with PC and underwent a debulking surgery but had complete remission under systemic treatment.
BC most commonly metastasizes to the bone, lung, liver, skin, soft tissue, adrenals and brain. Also, invasive lobular BC may metastasize to atypical intra-abdominal areas (peritoneum, gastrointestinal tract and adnexa). Notwithstanding, the presence of intra-abdominal disease adversely affects overall survival in BC patients. On the other hand, the average life expectancy was reported approximately 18 months. 5-year survival rate in patients with stage IV BC was found to be around 13%. The prognosis of BC patients with PC is considered to be lower than those who metastasize to other distant organ or tissues. However, BC cases with long-term survival were reported in recent years 1,2,3,4. Although the current guidelines do not recommend surgical treatment of intraabdominal metastases derived from BC, some oncology centers suggest surgical treatment, especially in patients with solitary metastases. The role of surgery in metastatic BC is controversial and currently, it is regarded as either palliative or of no benefit.
Recent advances in diagnostic technology and systemic treatment led to a significant improvement in the prognosis of BC patients. Therefore, with the prolongation of survival in BC patients, an increased number of cases with late recurrent PC should be expected. Late recurrence with PC should be considered when following patients with a history of BC. There are very few reports of BC patients with PC either as a synchronous or metachronous event. Therefore, there is no well established treatment for these rare cases. However, there were recent reports about treatment that provides long-term survival in BC patients with PC. But detailed treatment results were not reported. Therefore, no standard therapy was suggested. However, appropriate treatment for BC in the primary disease settings is mainly described, including multidisciplinary treatments such as surgery, CTX, endocrine therapy and molecular targeted medicine 6,7.
In their study, Panuta et al compared 19 female BC patients with intraabdominal metastases (peritoneal, hepatic, ovarian, etc.) in their series to the patients with similar features in other studies. The majority of stage IV BC patients treated in the unit were primary metastatic breast cancer cases with more adverse outcomes than cases with metachronous metastases. This fact explains the very low survival rates in patients in their cohort. The combination of targeted therapy and cytoreductive surgery, as well as the use of HIPEC in the treatment of metastatic breast cancer (with peritoneal carcinomatosis) is the subject of ongoing clinical trials 5. In their phase II study, Finn et al 8 found that adding palbociclib to letrozole significantly increased progression-free survival in these patients with HR-positive/HER2-negative cancer.
In conclusion, the probability of recurrence in patients with BC after multidisciplinary treatment may decrease with contemporary targeted treatments, but never disappears. It is expected that number of cases such as described here in this report will increase in time and with more experience on these cases, a standardized approach might be described in future 9,10. Therefore, oncologists and surgeons should take intraabdominal recurrences such PC under consideration for differential diagnosis when BC patients admit with gastrointestinal symptoms even after years. Even after incomplete resection by debulking surgery, long survival can be achieved in these patients by having complete remission with adequate systemic treatment.
Informed Consent
Kendisinden
References
- Fuke, A., Tabei, I., Okamoto, T. et al. Complete remission from peritoneal metastasis of late recurrent breast cancer by endocrine therapy: a case report. surg case rep 6, 313 (2020). https://doi.org/10.1186/s40792-020-01002-9
- Yu JH, Feng Y, Li XB, Zhang CY, Shi F, An SL, Liu G, Zhang YB, Zhang K, Ji ZH, Li B, Yan GJ, Li YP, Li Y. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for peritoneal metastasis from breast cancer: a preliminary report of 4 cases. Gland Surg. 2021 Apr;10(4):1315-1324. doi: 10.21037/gs-20-893. PMID: 33968683; PMCID: PMC8102231.
- Beniey M (August 11, 2019) Peritoneal Metastases from Breast Cancer: A Scoping Review. Cureus 11(8): e5367. doi:10.7759/cureus.5367
- DiPiro PJ, Tirumani SH, Cruz GP, Ramaiya NH, Lester SC, Shinagare AB. Lobular breast cancer: patterns of intraabdominal metastatic spread on imaging and prognostic significance. Abdom Radiol (NY). 2019 Jan;44(1):362-369. doi: 10.1007/s00261-018-1722-x. PMID: 30076430.
- Panuta, Andrian, et al. "Breast cancer with intraabdominal metastases. Is surgery necessary?" Archive of Clinical Cases, vol. 5, no. 4, Dec. 2018, pp. 128+. Gale Academic OneFile, link.gale.com/apps/doc/A573714396/AONE?u=anon~5d0d8984&sid=googleScholar&xid=ae3bb694. Accessed 25 Nov. 2021.
- Cardoso F, Costa A, Senkus E, Aapro M, Andre F, Barrios CH, et al. 3rd ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 3). Ann Oncol. 2017;28:3111.
- Wong, Y.M., Jagmohan, P., Goh, Y.G. et al. Infiltrative pattern of metastatic invasive lobular breast carcinoma in the abdomen: a pictorial review. Insights Imaging 12, 181 (2021). https://doi.org/10.1186/s13244-021-01120-4
- Finn RS, Crown JP, Lang I, Boer K, Bondarenko IM, Kulyk SO, et al. The cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole versus letrozole alone as first-line treatment of estrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): a randomised phase 2 study. Lancet Oncol. 2015;16:25–35.
- Spiliotis J, Ntinas A, Koustas P, Koupanis CH, Stefanopoulou, Dadoudis G. Breast Cancer Peritoneal Metastasis Role of Cytoreductive Surgery and HIPEC. Ann Surg Case Rep. 2021; 4(2): 1047.
- Caswell-Jin JL, Plevritis SK, Tian L, Cadham CJ, Xu C, Stout NK, Sledge GW, Mandelblatt JS, Kurian AW. Change in Survival in Metastatic Breast Cancer with Treatment Advances: Meta-Analysis and Systematic Review. JNCI Cancer Spectr. 2018 Nov;2(4):pky062. doi: 10.1093/jncics/pky062. Epub 2018 Dec 24. PMID: 30627694; PMCID: PMC6305243.
|