Abstract
Introduction: Bilateral thalamic and right mesencephalon infarct (BTMI) due to perioperative stroke is a rare and undesirable complication following surgery. Many risk factors cause perioperative stroke in clinical practice. We present the successful management of perioperative stroke following laparoscopic abdominal surgery in a patient with rectum cancer.
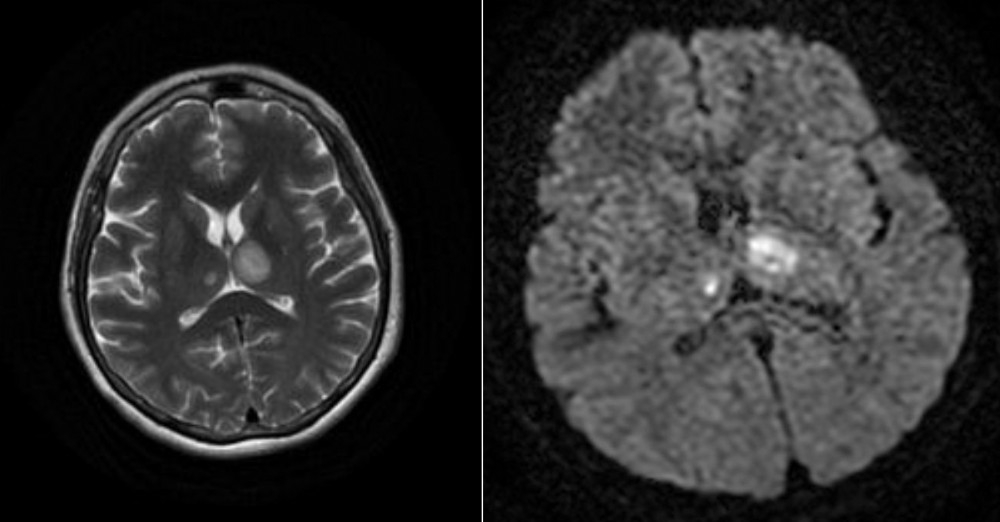
Case report: A 55-year-old female patient was admitted for rectum cancer. She had hypertension in her history. After evaluating the clinical and radiological findings, the patient underwent laparoscopic low anterior resection as total mesorectal excision with a loop ileostomy. The laparoscopic surgery was uneventful, and there was no intraoperative complication. The patient was taken to an intensive care unit and monitored. A lack of cooperation and mild disturbance of consciousness was observed on postoperative one day. A brain computed tomography, magnetic-resonance imaging, ultrasound, and echocardiography showed postoperative cerebrovascular stroke, including bilateral thalamic, right mesencephalon infarct, and nervous abducens injury after a postoperative follow-up. The neurology suggested low-molecular-weight heparin, clopidogrel, and duloxetine. She recovered slightly after medical treatment and was discharged on postoperative fourteen days. The patient is now in the postoperative 10th month with no neurological sequelae.
Discussion: A bilateral thalamic and right mesencephalon infarct due to perfusion is a significant complication. After general anesthesia in laparoscopic cancer surgery, cerebrovascular disease can occur. Early diagnosis and treatment of perfusion stroke can reduce morbidity.
Conclusion: A multidisciplinary approach is essential to manage bilateral thalamic infarct following general anesthesia in laparoscopic low anterior resection for rectum cancer.
Keywords :
Thalamic infarct
, laparoscopy
, low anterior resection
, perioperative stroke
, rectal cancer
Turkish Abstract
Giriş: Perioperatif inmeye bağlı bilateral talamik ve sağ mezensefalon enfarktüsü (BTMI), cerrahi sonrası nadir görülen ve istenmeyen bir komplikasyondur. Birçok risk faktörü klinik pratikte perioperatif inmeye neden olmaktadır. Rektum kanserli bir hastada laparoskopik batın cerrahisi sonrası perioperatif inmenin başarılı yönetimini sunuyoruz.
Olgu sunumu: 55 yaşında bayan hasta rektum kanseri nedeniyle başvurdu. Özgeçmişinde hipertansiyon vardı. Klinik ve radyolojik bulguları değerlendirildikten sonra hastaya loop laparoskopik low anterior rezeksiyon, total mezorektal eksizyon ve ileostomi açılması uygulandı. Laparoskopik cerrahi sorunsuz geçti ve intraoperatif komplikasyon gelişmedi. Hasta ameliyat sonrası yoğun bakım ünitesinde takibe alındı. Ameliyat sonrası birinci gün kooperasyon eksikliği ve hafif bilinç bozukluğu gözlendi. Beyin bilgisayarlı tomografisi, manyetik rezonans görüntüleme, ultrason ve ekokardiyografi, postoperatif takip sonrasında bilateral talamik, sağ mezensefalon enfarktüsü ve sinir abdusens yaralanması dahil olmak üzere postoperatif serebrovasküler inme geliştiği tespit edildi. Nöroloji, düşük moleküler ağırlıklı heparin, klopidogrel ve duloksetin önerdi. Medikal tedavinin ardından bir miktar iyileşti ve postoperatif ondört gün taburcu edildi. Hasta şu anda ameliyat sonrası 10. ayda ve herhangi bir nörolojik sekel yok.
Tartışma: Perfüzyona bağlı bilateral talamik ve mezensefalon enfarktüsü önemli bir komplikasyondur. Laparoskopik kanser cerrahisinde genel anestezi sonrası serebrovasküler hastalık oluşabilmektedir. Perfüzyona bağlı inmesinin erken teşhisi ve tedavisi morbiditeyi azaltabilir.
Sonuç: Rektum kanseri için laparoskopik low anterior rezeksiyonda genel anesteziyi takiben bilateral talamik enfarktüs tedavisinde multidisipliner bir yaklaşım esastır.
Turkish Keywords :
, Talamik infarkt
, laparoskopi
, low anterior rezeksiyon
, perioperatif inme
, rektum kanseri
Introduction
Colorectal cancer (CRC) is a severe health problem worldwide, and it is currently the third most common cancer and the leading cause of cancer-related deaths in the United States1. After the diagnosis of CRC, en-bloc surgery with adequate lymphadenectomy is a curative treatment in local or resectable CRC patients2. Although surgery is the primary modality in selected cases, it can be associated with complications such as hemorrhage, anastomotic leak, surgical site infection, and perioperative stroke (POS). Bilateral thalamic and mesencephalon infarct (BTMI) due to POS is rare after colorectal surgery for rectal cancer in clinical practice3. Bilateral thalamic infarct is 0.6% of all cerebral infarctions3. These cases generally have impairment of consciousness, diplopia, sleepness, cognitive disturbances, and atypical observable symptoms4. After diagnosing BTMI in magnetic resonance imaging, medical treatments such as low-molecular-weight heparin, clopidogrel, and duloxetine are essential for clinical courses5. We aim to present the successful management of the BTMI duo to POS following laparoscopic low anterior surgery.
Case Report
A 55-year-old female patient was admitted with a complaint of rectal bleeding for rectum cancer. The patient had hypertension and no smoking, alcohol, coagulant disorder, or coronary artery thrombosis anamnesis in history. The laboratory's hemoglobin, iron, and carcinoembryonic antigen (CEA) were ten g/dl, level 26 µg/dl, and 56.5 µg/dl. Colonoscopy showed rectum cancer with partial obstruction. After anesthesia consultation, she underwent laparoscopic low anterior resection with a loop ileostomy. The laparoscopic surgery was uneventful, and there was no intraoperative complication during surgery and anesthesia. The patient was taken to an intensive care unit and monitored.
On the first postoperative day, a lack of cooperation delayed awakening after general anesthesia, mild disturbance of consciousness, hypersomnia, and vision defect occurred. Typical signs were vertebral carotid artery doppler ultrasonography and computed tomography (CT). MRI diffusion revealed the acute ischemic process in the right half of the fourth ventricle and the right posterior cerebral artery area circulation. Moreover, a contrast-enhanced MRI demonstrated the acute ischemia that shows diffusion restriction in bilateral thalamus and right mesencephalon levels. Neurology confirmed BTMI with nervous abducens and suggested low-molecular-weight heparin, modafinil of 100 mg, clopidogrel of 75 mg, and duloxetine of 30 mg. The patient recovered slightly after anticoagulant treatment and was discharged with a mild level of neurological sequelae postoperative fourteen days. She followed up on neurology and oncology polyclinics. After several months, the patient is in the postoperative 10th month, and there are no neurological sequelae.
Discussion
CRC is a significant malignancy that can cause morbidity and mortality in the postoperative period or late diagnosis. An annual incidence of CRC is approximately 30-45/1000001. Although surgery is the primary treatment approach, some crucial complications can occur, no matter how many precautions2. Most critical difficulties lead to patients or operations, and an infarct following surgery, especially under general anesthesia, can cause several morbidity and mortality. Perioperative stroke (POS) is an emergency and life-threatening clinical entity that requires early diagnosis and treatment3. Bilateral thalamic infarction should be considered in the differential diagnosis of POS3,4. Bilateral thalamic and right mesencephalon with nervous abducens injury infarct following general anesthesia is extraordinary for rectal cancer.
Some risk factors include hypercoagulopathy, cardiac emboli, oral contraceptives, pregnancy, dehydration, vasculitis, inflammatory bowel disease, malignancy, systemic infections, genetic mutations, and coagulation factor deficiency can cause cerebrovascular infarction or thrombosis4,5. Furthermore, a cardiac embolism is a significant risk factor associated with bilateral thalamic infarcts6,7. On the other hand, hypothermia, metabolic disturbances, relative or absolute overdosage of medications, and anesthetics agents can occur during perioperative strokes7. Therefore, it has suggested an interdisciplinary approach to prevent complications. Nonetheless, in the present case, there was no risk factor such as coagulation disorder, obesity, smoking, or drug use to cause BTMI.
Four perforated arteries nourish the thalamus. First, thalamogeniculate arteries arising from the P2 segment of the posterior cerebral artery (PCA) maintain the lateral part of the thalamus. Second, the polar artery originated from the posterior communicant artery (PcoA), which provides blood to the anterior part of the thalamus. Third, the thalamoperforate (paramedian) arteries emerge from the P1 segment of the PCA to irrigate the medial aspect of the thalamus. Finally, the posterior choroidal artery arising from the PCA provides blood supply to the pulvinar, posterior thalamus, and geniculate bodies8. As a result, different clinical symptoms and signs occur in ischemia/infarct or perfusion dysfunction9. Bilateral thalamic infarct develops in 75% of paramedian (paramedian artery) and 44% of inferolateral (thalamogeniculate artery) area3,9. A classic triad of paramedian thalamic infarction consists of acute changes in consciousness, neuropsychological disorders, and vertical gaze disorders.
Moreover, lethargy, stupor, and hypersomnolence may be seen. Patients can be awakened, but they begin to fall asleep as soon as the stimulus ceases. Consciousness disorders are due to the involvement of the rostral mesencephalon and intralaminar nuclei. There may be vertical gaze disorders in which upward gaze paralysis is frequently seen. Neuropsychological anomalies, such as disorientation, apathy, apathy, anterograde amnesia, and recent memory defects and confabulations, can be observed in clinical practice. In infarcts involving the right medial thalamus, visual neglect, and constructional apraxia can be seen on the left. The findings are similar in bilateral thalamic infarcts, but they are more severe and permanent3,9,10. In the present case report, her arterial pressure and other parameters were normal during surgery. However, a lack of cooperation, mild consciousness disturbance, and vision defect occurred on the first postoperative day.
Computed tomography and MRI are required to diagnose BTMI. In 1983, Guberman et al. diagnosed BTMI by CT and clinical examination11. In addition, Lepore et al. showed the result of autopsy and MRI findings12. However, a CT is not more sensitive to diagnosis in the acute process of BTI. So, primarily, MRI is suitable and effective in the first hours of clinical symptoms12.
Management of BTMI has required early diagnosis and treatment. Postoperative perfusion thalamic and mesencephalon infarct have a good prognosis if early diagnosis and treatment begin. Anticoagulants Low-molecular weight-heparin and clopidogrel have been recommended in medical treatment12. Furthermore, modafinil can be effective for sleepiness due to narcolepsy.
Acknowledgement
There is no financial and commercial support, translation, statistics, technical support for graphics, tables, and figures. Informed Consent
Hastadan onam alındı
References
- Siegel RL, Miller KD, Jemal A. Cancer statistics. CA Cancer J Clin. 2019; 69(1): 7-34.
- Aziret M et al. Morbidity and long-term results in patients with wild and mutant type Kirsten rat sarcoma viral oncogene homolog (KRAS) mutations undergoing colorectal cancer surgery. Ann Ital Chir. 2022; 93(1): 65-77
- Kumral E et al. Clinical, etiological and MRI correlates. Acta Neurol Scand 2001; 103(1): 35-42.
- Lazzaro NA, et al. Artery of Percheron infarction: imaging patterns and clinical spectrum. AJNR Am J Neuroradiol 2010; 31(7): 1283-9.
- Ferro JM, Canhao P. Cerebral venous sinus thrombosis: update on diagnosis and management. Curr Cardiol Rep. 2014;16(9):523.
- Cassourret G, et al. Ischemic Stroke of the Artery of Percheron with Normal Initial MRI: A Case Report. Case Rep Med. 22010;2010:425734.
- López-Serna R, González-Carmona P, López-Martínez M. Bilateral thalamic stroke due to occlusion of the artery of Percheron in a patient with patent foramen ovale: a case report. Journal of Medical Case Reports. J Med Case Rep. 2009 Sep 15;3:7392.
- Carrera E, Bogousslavsky J. The thalamus and behaviour. Neurology. 2006; 66(12):1817-23.
- Çevik E, et al. Death Sleep at Emergency Department: Bilateral Thalamic İnfarct AKATOS. 2011; 2(4): 26-29
- Engelborghs S, et al. Loss of Psychic Self-Activation After Paramedian Bithalamic Infarction. Stroke 2000; 31(7): 1762-1765.
- Guberman A, Stuss D The syndrome of bilateral paramedian thalamic infarction. Neurology 1983;33(7): 540–546.
- Lepore FE, Gulli V, Miller DC. Neuro-ophthalmological findings with neuropathological correlation in bilateral thalamic-mesencephalic infarction. J Clin Neuroophthalmol 1985;5(4): 224–228.
Information Presentation
38. ulusal gastroenteroloji haftası ve gastroenteroloji cerrahisi kongresinde, Antalya, 16-21 Kasım.
|