Abstract
The tip of appendicitis may cause adhesion together with inflammation and rarely, it may cause small bowel obstruction by forming annular appendicitis. Rarely ever, cyclic appendicitis can cause perforation of the small bowel. We presented a case of perforation of 1.5'cm in the ileocecal region due to annular appendicitis, which has not been found in the literature
Keywords :
annular appendicitis
, small bowel
, obstruction
, adhesion
, perforation
,
Turkish Abstract
Apandisitin inflamasyonlu ucu, adezyona ve nadir de olsa halkalı apandisit oluşturarak ince bağırsak obstrüksiyonuna sebep olabilir. Bazen halkalı apandisit çok çok nadir de olsa ince bağırsak perforasyonuna neden olabilir. Biz, literatürde hiç bulunmayan halkalı apandisite bağlı ilioçekal böldede 1.5 cm'lik perforasyon vakasını sunduk.
Turkish Keywords :
, annüler apandisit
, ileum
, perforasyon
Introduction
In 1901, Hotchkiss et al. have firstly reported a patient who had small bowel obstruction after acute appendicitis1. However, until today, a very limited number of cases have been observed in the literature in which appendicitis caused small bowel obstruction. The appendicitis ring depends on the result of adhesion that develops after inflammation 2. Distal ileum perforation due to appendicitis ring could not be found in the literature. Because the two diseases are intertwined, the findings of small bowel obstruction may be prominent in the patients 2. Preoperative diagnosis may not be made to explain this picture, and the diagnosis is usually intraoperative. In such cases, prompt diagnosis and treatment are important in terms of patient morbidity and mortality.
Case Report
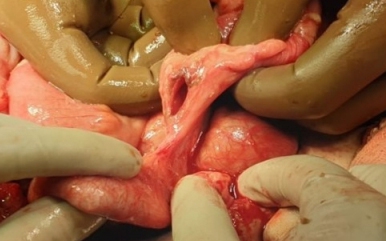
A 22-year-old female patient applied to our clinic with complaints of nausea, abdominal pain for 2 days, and vomiting in the last hours. On physical examination, abdominal tenderness and rebound were positive. No pathological findings were found in rectal examination. In laboratory values, wbc (12.56 /μL) and neutrophilia (% 88.3) were at high levels. Whole Abdominal Computed Tomography (with contrast): In Douglas, free fluid was noted in both paraovarian areas, diffuse between the pelvic bowel loops, and also observed in the perihepatic and perisplenic area. The patient was operated under emergency conditions considering perforation due to widespread tenderness and rebound observed on physical examination and free fluid observed on tomography. Midline laparotomy was performed on the upper and lower parts of the umbilicus. After the abdomen was opened, dirty fluid was observed in it. In the exploration, it formed an annular internal hernia by adhesion to the tip of the appendix and wrapping the ileum 2 cm proximal to the annular ileocecal valve (Figure 1).
A perforated area of 1.5 cm was observed in the antimesenteric area of the ileum, just proximal to the appendicular ring (Figure 2).
The appendix was approximately 4 cm long and a fibrous extension of the adhesion was observed at its tip. Appendectomy was performed (Figure 3).
Its pathology was reported as suppurative appendicitis. Lembert sutures were placed in the perforated area of the small intestine with full-thickness 3/0 polyglactin and then with seromuscular 3/0 polypropylene. He was discharged without any problems one week later.
Discussion
Acute appendicitis is the most common of the acute abdominal emergencies. Since the appendix is free, mobile, and in various forms, it can adhere to the neighboring organs with adhesion in its inflammation, and even form a ring around it with adhesion and obstruct the organ. Chowdary has stated in 2016 that the tip of the appendix wraps around and adheres to the small intestine in the form of a ring and this is a rare pathological condition3 .
The diagnosis is usually made intraoperatively4 . Appendicitis findings are suppressed, and ileus findings generally dominate the picture. Perforation in the proximal of the obstruction, which is even less common, may make the diagnosis more difficult. However, it could not be diagnosed by tomography that the perforation developed due to the appendicular ring. The presence of diffuse intra-abdominal fluid in the tomography and the inability to produce gas and stool in the physical examination, the absence of bowel sounds, tenderness, and rebound findings made us think that the patient had perforation and perform emergency surgery.
Small bowel obstruction of acute appendicitis can usually develop after appendicitis inflammation causes small bowel ileus, with appendix tumor, after appendix perforation or abscess that develops due to appendix perforation5 . Small bowel obstruction caused by inflammation of the appendix, which causes ring formation, is very rare. Only a few case reports have been found in the literature6. Moreover, in our case, there was small bowel obstruction due to suppurative acute appendicitis and perforation just proximally.
Conclusion
Small bowel perforation due to the appendicular ring in suppurative appendicitis is very limited in number in the literature. In general, obstruction and perforation due to the appendicular ring are observed intraoperative. Perforation due to various reasons, originating from the intra-abdominal gastrointestinal organs, is observed, and it should be kept in mind that there may be, very rare, perforation of the small intestine due to the appendix ring. Therefore, prompt diagnosis and treatment are always essential.
Informed Consent
From the Patient
References
- Hotchkiss L. Acute intestinal obstruction following appendicitis. a report of three cases successfully operated upon. Ann Surg.1901;34: 660-677.
- Harrison S, Mahawar K, Brown D, Boobis L, Small P. Acute appendicitis presenting as small bowel obstruction: two case reports. Cases J. 2009;2(9):106.
- Chowdary PB. Appendicular tourniquet: a cause of intestinal obstruction. J Clin Diagn Res. 2016;10 (5):9–11.
- Lawani İ, Houndje C.Y.P, Souaïbou Y.I, Gbéssi D.G,Attolou S.G.R, Gnangnon F.H.R., Komadan K.S., Koco H.,Dossou F.M, and Togbé J.O.Internal hernia strangulated on appendicular tourniquet: a case report of an exceptional anomaly of the appendix revealed by a rare hernia. Lawani et al. Surgical Case Reports. 2019; 5:112.
- O'Donnell M.E, Sharif M.A, O'Kane A, Spence R.A. Small bowel obstruction secondary to an appendiceal tourniquet. Ir J Med Sci. 2009;178(1):101-05.
- Assenza M, Ricci G, Bartolucci P, Modini C. Mechanical small bowel obstruction due to an inflamed appendix wrapping around the last loop of ileum.G Chir. 2005;26(6-7):261-66.
|