Abstract
Schwannomas are tumors of the peripheral nerve sheath, usually seen in the head and neck region, and rarely in the retrorectal area. The case is here presented of a retrorectal schwannoma, which was detected incidentally during examination for cholelithiasis, resected with a combination of transabdominal and posterior sacral approaches. The optimal surgical treatment of masses in the presacral region is total resection of the mass. If the distal part of the lesion can not be reached during transabdominal surgery, the entire mass can be removed by adding the posterior sacral approach.
Keywords :
presacral mass
, schwannoma
, surgical extirpation
Turkish Abstract
Schwannomlar periferik sinir kılıfından oluşan ve retrorektal alanda nadiren görülen tümörlerdir. 45 yaşındaki erkek hastanın tetkiklerinde presakral alanda 10 cmlik kitle gözlenmesi üzerine operasyon kararı alınmıştır. Ameliyat sırasında trans abdominal yolla kitle sakrumdan ayrılamamış ve posterior yaklaşım kararı alınmıştır. Koksiks çıkarıldıktan sonra kitleye posteriordan ulaşılmış ve kitle presakral alandan tamamen serbestleştirilmiştir. Sonrasında kitle batından çıkarılmıştır. Presakral bölgedeki kitlelerin optimal cerrahi tedavisi kitlenin total rezeksiyonudur. Transabdominal yoldan yapılan cerrahi sırasında lezyonun distaldeki kısmına ulaşılamaz ise posterior yaklaşım da eklenerek kitlenin tamamı çıkarılabilir.
Turkish Keywords :
, presakral kitle
, schwannom
, cerrahi ekstirpasyon
Introduction
Schwannomas, previously known as neurinoma, was first described by Verocay in 1908 1. Schwannomas due to the proliferation of nerve sheath cells are slow growing and rarely malignant tumors. These are the second most common peripheral nerve tumor after neurinomas 2, are usually benign, and seen in adulthood with no gender difference. Schwannomas are almost always seen as solitary lesions because of the slow growing nature of the tumor so pain and neurological symptoms are the last symptoms to appear 3. Retrorectal schwannomas are generally detected during abdominal examination or rectal examination. However, they may present with chronic pelvic and back pain, impotence, lower extremity pain, urinary incontinence or retention and renal colic symptoms 4.
In this paper, the case is presented of resection of a giant retrorectal schwannoma, which was detected incidentally during examination for cholelithiasis and choledocholithiasis, and to the intervention was made with a combination of the transabdominal and posterior sacral approaches.
Case Report
A 45-year old male was admitted to the Gastroenterology Outpatient Clinic for endoscopic retrograde cholangiopancreatography (ERCP) due to choledocholithiasis. A 10 x10 cm mass was observed in the presacral area on control ultrasound imaging and the patient was referred to the Gastroenterology Surgery Outpatient Clinic. Abdominopelvic computed tomography showed a solid mass in the presacral area of approximately 10 x10 cm with heterogeneous density without invasion of surrounding structures (Figure 1).
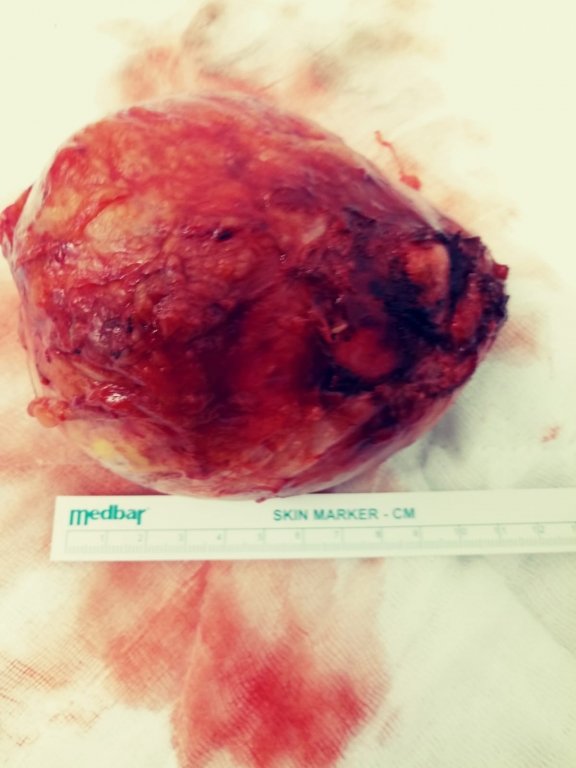
No intraluminal mass was observed on sigmoidoscopy. The laboratory parameters and tumor markers were normal. The patient was admitted for surgery. After the median incision, the mass of approximately 15 cm was detected, beginning from the presacral area, the rectum was deviated laterally, and there was no invasion of the bladder or surrounding tissues. The mass was separated from the surrounding tissues, but was seen to be attached to the presacral area. Due to the location of the mass, it was decided to also apply a posterior sacral approach. With the patient in the supine position turned to jack-knife position, an elliptical incision was made through the sacrum. The sacral incision was closed after removal of the coccyx and the mass was completely separated from the presacral area. The patient was returned to the supine position and the mass was then removed through the abdomen. The patient was also applied with cholecystectomy, and the histopathology report was of schwannoma, 13x10x8 cm in size (Figure 2).
Discussion
Tumors in the presacral area are rare and diagnosis can be delayed because of the non-specific symptoms. Tumor size is usually 5-6 cm, and larger ones can be seen at the rate of 0.3-5%, often in a retroperitoneal location 3. Although most of the retrorectal masses are congenital, the majority of patients do not have a family history. They are usually detected incidentally during proctological examination. In rectal examination, 97% of retrorectal masses can be palpated 5. Sigmoidoscopy is used to evaluate rectal invasion of the mass. Transrectal ultrasound is 100% sensitive and provides information on tumor size and invasion. Computed tomography can evaluate even small lesions, differentiate between solid and cystic lesions and evaluate sacrum and peripheral organ invasion. Magnetic resonance imaging is used for the evaluation of soft tissues and the relationship between tumor and sacrum and nerves 6. Diagnostic biopsy is only used to plan adjuvant therapy for inoperable or locally advanced tumors 7.
Histopathologically, schwannomas are usually solid encapsulated tumors. Although cystic degeneration is most commonly seen (66%), there may also be calcific, hemorrhagic and hyaline degeneration, but malignant degeneration is not usual. There are two histological types in schwannomas: Anthony A pattern with frequent and parallel alignment of spindle cells and Antony B pattern with long or oval nuclei associated with cytoplasm 2.
Treatment of presacral schwannomas is en bloc removal of the mass using transabdominal, posterior sacral or combined methods. The method to be used is determined by the location of the mass in the sacrum and the size of the mass 4. Retrorectal tumors above the level of S3 are traditionally excised transabdominally, whereas the posterior sacral method may be preferred in small lesions below S3 level 8. Abernathey et al. reported that tumor recurrence was observed in 54% of patients who underwent intralesional curettage and re-operation was required. It was concluded that radical resection with surrounding tissues was necessary to reduce the recurrence of schwannomas in the sacrum 9. Active bleeding may be present if the tumor capsule adheres to the presacral venous plexus after radical surgery 10.
In conclusion, although schwannomas are mostly observed in the extremities, they should be kept in mind when patients present with a mass in the presacral region. Retrorectal schwannomas require radical resection to prevent recurrence. If the mass cannot be completely removed with an anterior approach, the posterior approach can help to obtain radical resection of the mass.
References
- Schindler OS, Dixon JH. Retroperitoneal giant schwannomas: report on two cases and review of the literature. J Orthop Surg 2002;10:77-84.
- Ozkan OF, Celik AS, Koksal N et. all. Angiographic Embolization and Excision in Patient with Giant Retrorectal Schwannoma. Kolon Rektum Hast Derg 2011;21:136-140.
- Erdem H, Cetinkunar S. Presacral giant schwannoma: A case report and review of the literature. Dicle Medical Journal 2015; 42 (1): 107-110.
- Santiago C, Lucha PA. Atypical Presentation of a Retrorectal Ancient Schwannoma: A Case Report and Review of the Literature. Military Medicine 2008;173(8):814-6.
- Schleinstein HP, Curiati PAL, Averbach M et. all. Retrorectal Tumor: A Case report of a patient with schwannoma. ABCD Arq Bras Cir Dig 2015;28(2):151-152.
- Baek SK, Hwang GS, Vinci A et. all. Retrorectal Tumors: A Comprehensive Literature Review. World J Surg 2016; 40(8):2001-15.
- Buchs N, Taylor S, Roche B. The posterior approach for low retrorectal tumors in adults. Int J Colorectal Dis 2007;22:381?5.
- Witherspoon P,Armitage J, Gatt M et al. Laparoscopic Excision of Retrorectal Schwannoma. Dis Colon Rectum 2010; 53: 101?3.
- Abernathey CD, Onofrio BM, Scheithauer B et al. Surgical management of giant sacral schwannomas. Journal of Neurosurgery 1986;65(3):286?95.
- Samarakoon L , Weerasekera A, Sanjeewa R et al. Giant presacral schwannoma presenting with constipation: a case report. Journal of Medical Case Reports 2012;6:285-8.
|