Abstract
Congenital cholesteatoma is a pathology that is thought to arise from embryonic remnants or inclusions but the mechanism of evolution of is not fully understood. Genetic factors, mastoid cavity pneumatization and the temporal bone developmental anomalies are considered to be effective in the formation of the congenital cholesteatoma. Although, anteriorly displaced sigmoid sinus is common, a sigmoid sinus which fills the whole mastoid cavity is a rarely seen anatomical variation. Herein, we reported a patient with these two rare conditions, namely sigmoid sinus which filled the whole mastoid cavity and congenital cholesteatoma was presented. We think that this case report will contribute to medical literature and aid professional practice.
Keywords :
Congenital Cholesteatoma
, Sigmoid Sinus
, Anatomical Variation
, Mastoid Cavity
Turkish Abstract
Konjenital kolesteatom embriyonel epitelyal kalıntılardan ya da inklüzyonlardan meydana geldiği düşünülen ancak oluşum mekanizmasının tamamen açıklanamadığı bir patolojidir. Konjenital kolesteatom gelişiminde genetik faktörler, mastoid havalanma ve temporal kemik gelişim anomalilerinin etkili olabileceği ileri sürülmektedir. Anterior yerleşimli sigmoid sinüs sık rastlanabilen bir durum olmakla birlikte, sinüsün tüm mastoid kaviteyi dolduracak şekilde yerleşmesi oldukça nadir görülen bir anatomik varyasyondur. Olgumuzun bu nadir varyasyonu taşıması ve konjenital kolesteatom ile birlikte olmasının klinik tecrübe ve literatüre katkı açısından önemli olduğunu düşünmekteyiz.
Turkish Keywords :
, Konjenital Kolesteatom
, Sigmoid Sinüs
, Anatomik Varyasyon
, Mastoid Kavite
Introduction
Congenital cholesteatoma is a rare childhood disease that is generally detected incidentally in otological examination. Mostly, it is presented as a pearly white mass medial to the intact tympanic membrane especially at the anterosuperior and posterosuperior quadrants. It can be diagnosed in patients with no prior history of otorrhea, tympanic perforation, head trauma or previous otologic procedures. The most common presenting symptom is conductive hearing loss. Pathophysiology still remains unclear but epithelial rest theory is the most accepted one
Sigmoid sinus is one of the most important landmarks in otological surgeries. So, the position of the sinus is really crucial to avoid any unexpected complications during the operation. It can differ according to a prior chronic otitis media history or genetic factors that cause hypopneumatization, but the origin is still not clear. The location of the sinus can differ from patient to patient more then expected and anteriorly displaced sigmoid sinus is one of the most frequently seen variation. In our case mastoid cavity was filled with sigmoid sinus and at the same time the patient had congenital cholesteatoma. Herein, we present a patient with these two rare conditions because we think that this case will be useful both for the literature and clinical experience.
Case Report
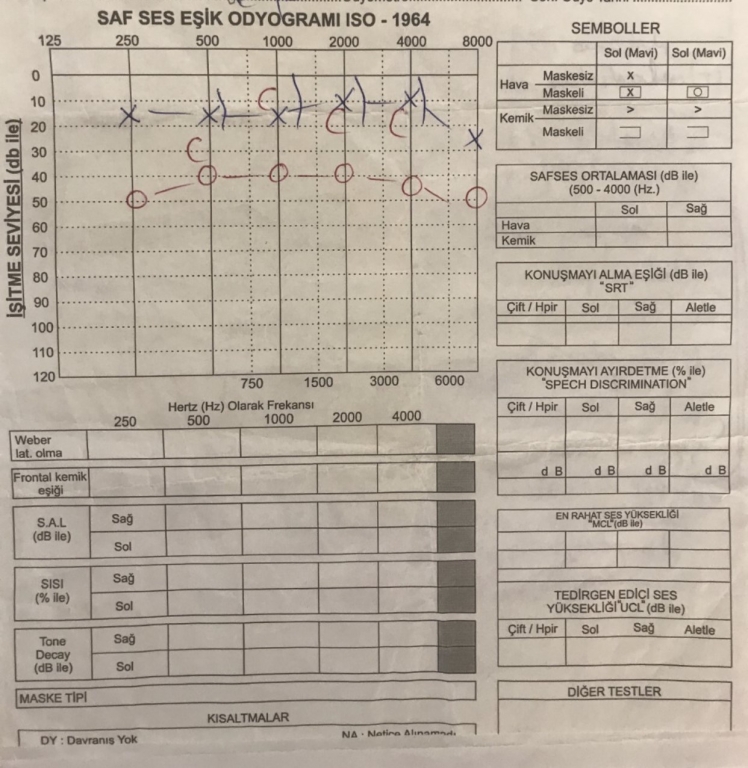
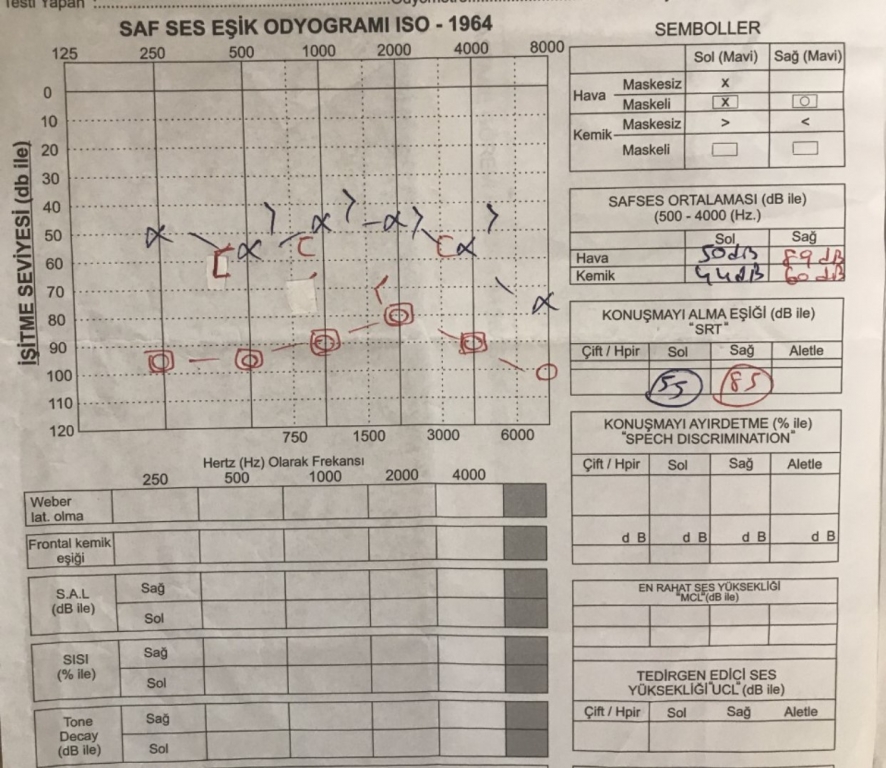
A 10-year-old male patient presented to Haseki Training and Research Hospital outpatient clinic with progressive hearing loss in his right ear. In the physical examination a white mass was seen behind the right tympanic membrane and it bulged towards the external ear canal. Both tympanic membranes were intact. External ear canals were also normal. The audiometry which was performed in 2018 demonstrated a conductive hearing loss with 30 decibel (dB) gap on the right side and a normal hearing on the left (Figure 1), while the new test which was performed in 2019 demonstrated a mixed type hearing loss on the right side with a 40 dB gap and a sensorineural hearing loss on the left side (Figure 2).
The temporal bone computerized tomography(CT) showed that the middle ear cavity was filled with soft tissue densities consistent with cholesteatoma and the bony structures like scutum and the ossicles were eroded(Figure 3).
Also on the right side sigmoid sinus was displaced abnormally anteriorly. After all these examinations we diagnosed it as a congenital cholesteatoma and scheculed a timpanomastoidectomy operation for the right ear.
Operation started with a retroauricular incision and mastoid cortex was exposed. Small number of aired cells started to be removed then we saw that the mastoid cavity was filled with sigmoid sinus and it was impossible to reach to mastoid antrum retroauricularly(Figure 4).
So, we changed the plan and continued with the inside-out technique. After the elevation of tympanomeatal flap, middle ear cavity was exposed and cholesteatoma was observed filling the whole middle ear cavity. We tried to identify the ossicles; incus long arm was eroded, there were no stapes and the malleus head was covered with cholesteatoma. First of all, incus was removed then atticotomy was performed. After that, canal wall down (CWD) procedure was performed and the malleus was removed to be sure that middle ear and antrum were cleared from all the cholesteatoma. The bone defect on the sigmoid sinus was reconstructed with a concal cartilage graft and after a meatoplasty, surgery was completed. No recurrence was detected on the follow-up at fifth month of recovery and the follow-ups still continue.
Discussion
Congenital cholesteatoma is a progressive growth of aberrant epithelial remnants in the middle ear cavity which generally ends up with destruction of the ossicles and bony structures of the temporal bone. Although, it is always indicated that the temporal bone is its most typical location, it can also present in the mastoid process, petrous bone, external ear canal and even intracranially 1. It is still accepted as a rare condition with an incidence estimated 12 per 100,000 kids but the reported cases are pretty much increased with the actual knowledge 2. Most often, it is caught around age 3 to 6 during a routine otological examination as a pearly white mass located medial to the intact tympanic membrane unilaterally without causing any symptoms 3. Approximately, 3 percent of all congenital cholesteatomas can be bilaterally so the examinations must be done carefully 4. Generally, the mass locates in anterosuperior quadrant but the ones which locate in posterosuperior quadrants should not be underestimated as frequency 5. As the mass grows and starts to affect the ossicular chain the most common presenting symptom is conductive hearing loss. Other presenting symptoms can be fasial paralysis or intracranial complications according to the delay of the diagnosis. When the mass extends to the ossicular chain, the incus is the most commonly affected one, which is followed by the stapes superstructure 1. These patients do not have prior history of otorrhea, timpanic perforation, trauma or otological procedures so theoretically these patients are considered to have a normal ear structure. Marchioni et al., reported that patients with congenital cholesteatoma had well pneumatized mastoid cells compared to the chronic otitis media patients with cholesteatoma 6. But, in our case, even though, the patient did not have a history of otitis media, his mastoid cells were poorly pneumatized.
The only treatment is surgery. According to the extensivity of the disease transcanal endoscopic approach (TEA), retroauricular canal wall up (CWU) or CWD mastoidectomies must be choosen. Some authors prefer TEA for preserving the normal structure of the middle ear as much as they can while having a good view of the hidden areas and reduce the risk of residual cholesteatoma and in extensive cases they prefer to combine it with microscobic CWU mastoidectomy 6. On the other hand, in extensive cases some authors suggest CWD mastoidectomy as the best way to eradicate the disease, while some of them totally avoid this procedure. The reason is with a meatoplasty the patients quality of life is decreased, they should prevent their ear from water for life and frequently have to have hospital visits to clean the cavity. Because of young age these kind of restrictions are hard to accomodate 6. In our case the middle ear cavity was filled with cholesteatoma and it was imposibble to eradicate the disease without performing CWD mastoidectomy.
Sigmoid sinus is one of the most important landmarks in otological surgeries. It is a S-shaped dural venous sinus that extends beneath the temporal bone from the mastoid process to the jugular foramen. It forms the posterior border of the mastoid cavity so different presentations of the sinus affect the surgical approach. Most commonly, it is displaced anteriorly due to the hypopneumatization of the mastoid or a chronic otitis media history causing sclerosis in the mastoid bone 7. But the cause of this anatomical variation is still not clear. There are few reported cases about this anatomical variation; Addeen et al., reported a case with a massive bleeding of an anteriorly displaced sinus as a complication of a myringoplasty7, while Ulug et al., Ulug referanslar arasında göremedim. Ben ekledim.. reported a stapedectomy case with the same complication 8. In our case, the sigmoid sinus was also anteriorly displaced but most importantly it was filling the whole mastoid cavity inhibiting the routine antrotomy approach so we had to continue with inside-out technique.
Conclusion
Anatomical variations of the sigmoid sinus are frequent then we expect. The surgeons should be prepared of such variations to prevent any intraoperative complications. Temporal bone CT is a very useful imaging technique to warn the surgeon preoperatively. Otherwise, unexpected fatal bleedings might occur. In our case, mastoid cavity was filled with sigmoid sinus and at the same time the patient had congenital cholesteatoma. Herein, we report the existence of these two rare disorders in a single patient because we think that this case report will contribute to medical literature and aid professional practice.
References
- Mostafa B E, Lobna E F. Congenital cholesteatoma: the silent pathology. Otorhinolaryngol Relat Spec. 2018; 80 (2): 108-16.
- Walker D, Shinners M J. Congenital Cholesteatoma. Pediatr Ann. 2016;45 (5): e167-e170.
- Morita Y, et al. Pediatric middle ear cholesteatoma: the comparative study of congenital cholesteatoma and acquired cholesteatoma. Eur Arch Otorhinolaryngol. 2016;273 (5): 1155-60.
- Lee C H, et al. Bilateral congenital cholesteatoma. Otol Neurotol. 2018;39 (5): e336-e341.
- Kansu L, Ozluoglu LN. Congenital cholesteatoma together with ossicular chain anomaly. Eur Arch Otorhinolaryngol. 2017; 274 (2): 1179-82.
- Marchioni D, et al. Bilateral congenital cholesteatoma: Surgical treatment and considerations. Internat Pediatr Otorhinolaryngol. 2017;99: 146-51.
- Addeen S Z, Al-Mohammad M. An abrupt bleeding of the anteriorly-displaced sigmoid sinus: a rare complication of myringoplasty. BMC Ear, Nose and Throat Disord. 2017 ;12 (17): 12.
- Ulug T, et al. An unusual complication of stapes surgery: profuse bleeding from the anteriorly located sigmoid sinus. Eur Arch Otorhinolaryngol. 2004;261(7):397-9.
Information Presentation
41th Turkish National Otorhinolaryngology and Head and Neck Surgery Congress. Poster presentation. 13-17 November, 2019 Antalya, Turkey
|