Abstract
Parathyroid carcinoma is a rare disease that accounts for approximately 1% of all hyperparathyroidism cases. It is an endocrine disease, characterized by severe hyperparathyroidism with unknown aetiology. In this article, we present two cases diagnosed and treated with parathyroid carcinoma. Two female patients, 55 and 41 years old, presented with fatigue and diffuse bone pain. The serum calcium of the 55-year-old patient was 11.4 mg/dL and the parathormone was 1900 pg/mL. Examination revealed a solid lesion with a diameter of 32x27 mm in the right lower region of the neck. A 41-year-old patient had a serum calcium of 11.1 mg/dL and a parathyroid hormone of 2100 pg/mL. Examination revealed a solid lesion with a diameter of 35x29 mm in the left lower region of the neck. Parathyroidectomy was performed in both patients. Thyroid lobectomy was also performed in the second patient. Histopathological examination revealed parathyroid carcinoma. Calcium and parathormone levels decreased in the follow-up of both patients. In the second patient, radiotherapy was applied because the tumor was positive at the surgical margin. The only treatment for parathyroid cancer is surgery. When intraoperative large parathyroid gland and local invasion are detected, parathyroid cancer should be considered and extended surgical resection should be performed.
Keywords :
Parathyroid carcinoma
, hyperparathyroidism
, hypercalcemia
Turkish Abstract
Paratiroid karsinomu nadir görülen bir hastalıktır ve tüm hiperparatiroidizm vakalarının yaklaşık %1'ini oluşturur. Şiddetli hiperparatiroidizm ile karakterize olup, etyolojisi bilinmeyen endokrin bir hastalıktır. Bu çalışmada, paratiroid karsinomu tanısı almış ve tedavi edilmiş iki olguyu sunuyoruz. Ellibeş ve 41 yaşında iki kadın hasta, halsizlik ve yaygın kemik ağrısı şikayeti ile başvurdu. Ellibeş yaşındaki hastanın serum kalsiyumu 11.4 mg/dL ve parathormonu 1900 pg/mL idi. Tetkiklerinde boynun sağ alt bölgesinde 32x27 mm çapında bir lezyon saptandı. Diğer hastamız 41 yaşında olup serum kalsiyumu 11.1 mg/dL ve parathormonu 2100 pg/mL bulundu. Tetkiklerinde boynun sol alt bölgesinde 35x29 mm çapında sert bir lezyon saptandı. Bu lezyonlar paratiroid adenomu olarak düşünüldü. İlk hastamıza paratiroidektomi yapıldı. İkinci hastamıza ise hem paratiroidektomi hem de tiroid lobektomi yapıldı. Her iki hastanın da takibinde kalsiyum ve parathormon seviyeleri düştü. Histopatolojik incelemede paratiroid karsinomu oldukları saptandı. İkinci hastanın patoloji incelemesinde cerrahi sınırda tümör pozitif geldiği için, radyoterapi uygulandı. Beş yıllık takiplerinde nüks oluşmadı. Sonuç olarak; paratiroid kanseri için tek tedavi seçeneği cerrahi operasyondur. İntraoperatif büyük paratiroid bezi ve lokal invazyon tespit edildiğinde paratiroid kanseri göz önünde bulundurulmalı ve genişletilmiş cerrahi rezeksiyon yapılmalıdır.
Turkish Keywords :
, Paratiroid karsinomu
, hiperparatiroidizm
, hiperkalsemi
Introduction
Parathyroid carcinoma (PC) is one of the exceedingly rare endocrine tumours. It was first reported by Sainton and Millot in 1933. It accounts for 0.4-2% of all hypercalcemia cases 1. The aetiology of the disease has not been clarified yet 2. The disease is characterized by hypercalcemia and hyperparathyroidism. The morbidity and mortality associated with PC are related to the severity of hypercalcemia 3. Of all the patients with this disease, 10% have non-functional PC 4. It is difficult to diagnose the disease in the preoperative period and during surgery, because it is potentially misdiagnosed as a PC 2,3. In this article, we aimed to present our two patients with PC and discuss current information in the literature.
Case Report
Case 1: A 55-year-old female patient presented with fatigue and widespread bone pain. The physical examination revealed a palpable lesion in the right lower neck. The levels of calcium (Ca) and intact parathyroid hormone (PTH) were 11.4 mg/dL and 1900 pg/mL, respectively. In the ultrasound (US) examination, a solid lesion with a size of 32x27 mm was observed in the lower pole of the right thyroid lobe. This lesion was consistent with parathyroid adenoma. Tc-99m-sestamibi scintigraphy revealed findings suggesting that it might be a parathyroid adenoma. T-score was low with a value of -5 as determined in spine and pelvis bone densitometry. Parathyroidectomy was performed. No adhesion to surrounding tissues was observed during the operation. The lesion was sent to pathology. Pathological examination revealed parathyroid carcinoma with local invasion, capsular involvement, perineural invasion and large fibrous bands.
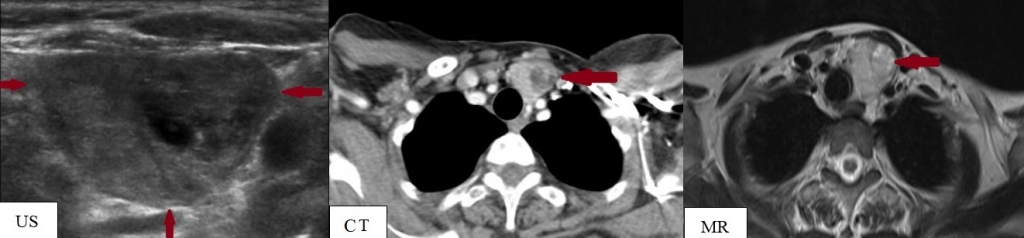
Case 2: A 41-year-old female patient presented with fatigue, widespread bone pain, and dyspepsia. In the physical examination, a solid lesion was found in the left lower neck. The Ca level was 11.1 mg/dL and the PTH level was 2100 pg/mL. In the neck US, a 35x29 mm sized, lobulated solid lesion located in the lower pole of the left lobe of the thyroid was observed. There were no pathological lymph nodes in the neck. In the neck sonography, differential diagnosis of parathyroid adenoma and parathyroid carcinoma could not be made. Neck computed tomography (CT) and neck magnetic resonance imaging (MRI) were performed to better identify the lesion characteristics and to determine lesion limits (Figure 1).
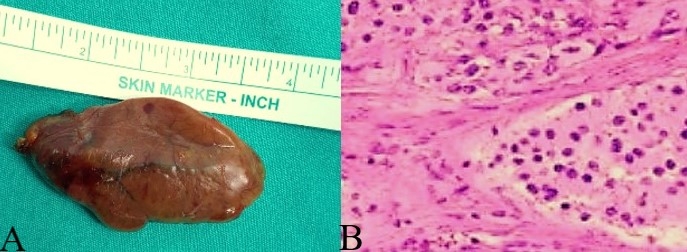
On CT and MRI, the lesion was attached to thyroid. However, there were no pathological lymph nodes. Scintigraphy findings were reported to be compatible with a parathyroid adenoma. T-score was low with a value of -7 as determined in spine and pelvis bone densitometry. Parathyroidectomy was performed. During surgery, the parathyroid lesion invading the thyroid tissue was easily separated from the surrounding muscle structures. There was no palpable lymph node. The lesion was extensively removed. Left thyroid lobectomy was performed. The lesion was sent to pathology. Pathological examination revealed parathyroid carcinoma (Figure 2) with local invasion, capsular involvement, perineural invasion, vascular invasion, large fibrous bands and necrosis.
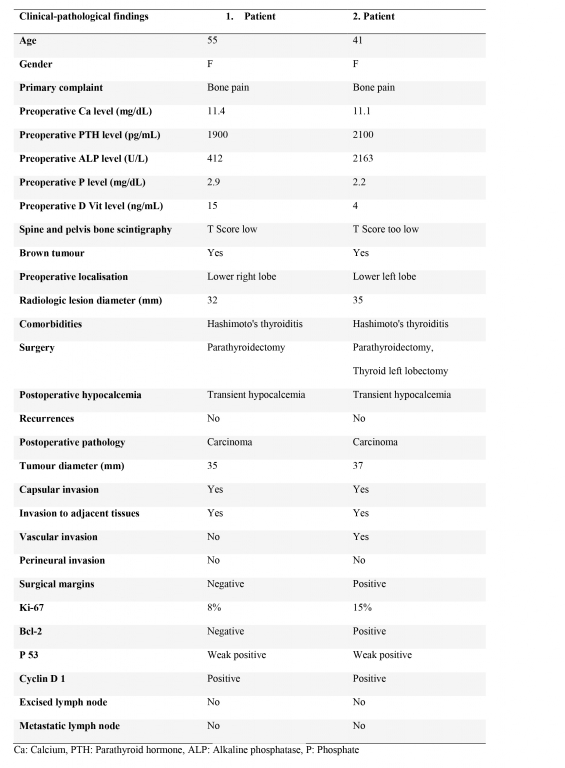
In both patients, the postoperative levels of Ca and PTH decreased. The pathological examination of patient-II revealed invasion of the tumour into the thyroid tissue, therefore, radiotherapy was given to the patient. No recurrences or metastases were detected in the 5-year follow-up of the patients. Clinical and pathological findings in the patients were summarized in Table 1. In this process, informed consent was obtained from the patients.
Discussion
Parathyroid carcinoma accounts for 0.4-2% of all hypercalcemias and 1-3% of all primary hyperparathyroidism cases 1,5. It is most common in the fourth and fifth decades of life. It is seen at equal rates in males and females 6. Our patients were both females in the fourth and the fifth decades of life.
Parathyroid carcinoma is thought to be formed by the interaction between genetic and environmental factors 6. It is reported that receiving radiotherapy at a young age and the presence of an end-stage renal disease are the predisposing factors1. The disease may also be seen in hyperparathyroidism-jaw tumour syndrome and multiple endocrine neoplasia (MEN) I and IIA syndromes 1-3.
Major abnormalities that involved in parathyroid carcinogenesis, include calcium sensing receptor (CaSr) activation disorder and disorders in cyclin D1 and Wnt/?-catenin signalling disorders. It is suggested that abnormalities in the inactivation of CaSr enhance cyclin D1 and Wnt/?-catenin signalling, leading to the development of hyperplasia, adenomas, and neoplasias in the parathyroid gland 7,8.
Mutations in CCND1/PRAD1 (11q13) and RET (10q11.2) proto-oncogenes have been found in PC at a rate of 90% and 5%, respectively, enhancing cyclin D1 signalling 5,7. CDC73/HRPT2 mutations were detected in more than 70% of sporadic PCs 8.
Fatigue, anorexia, weight loss, nephrolithiasis, bone pain, nausea, vomiting, pancreatitis, constipation, depression, cardiac arrhythmia, and rarely coma may occur 1. PC should be suspected if there is neck pain, a palpable mass in the neck, dysphagia, dysphonia, and a jaw tumour 3. Since 10% of PCs are nonfunctional without hyperparathyroidism, diagnosis is late. Patients usually present with a locally advanced cervical mass 4. The primary complaint was the bone pain in both of our patients.
Hyperparathyroidism (PTH level >3-fold), hypercalcemia (albumin-adjusted Ca >3.0 mmol/L), and the ratio of the third generation PTH to the second-generation PTH >1 indicate a PC 3,5. Increased levels of alkaline phosphatase, hypophosphatemia are observed more commonly1,3. The levels of PTH were >3-fold in both of our patients. Their hypercalcemia levels were <14 mmol/L.
In the US examination; the presence of calcifications, irregular margins, hypoechogenicity, and increased vascular pattern are interpreted suggesting a carcinoma. Tumour location was defined with Tc-99m-sestamibi scintigraphy 2. CT and MRI are used for detecting PC and metastases 3. Positron emission tomography can be used in order to perform preoperative staging and to detect recurrences or metastases in PC 1,2. A fine needle aspiration biopsy is not recommended as making the distinction between a malignant and benign tumour is difficult and it may cause contamination and spread of tumour cells 1,3,7.
The only treatment for PC is surgery. Ca levels >14 mg/dL should be reduced preoperatively. Cervical lymph node metastases are present in 15-30% of patients 6. Extended tumour resection is performed to reduce the risk of recurrences and increase life expectancy 7. If metastases are observed in the lateral lymph nodes, a modified radical neck dissection should be performed. It is necessary to protect the parathyroid capsule to prevent local recurrences 8,9. Parathyroid tumour excision with ipsilateral thyroid lobectomy and central lymph node dissection are performed.
Since, parathyroid tumours show a uniglandular cell proliferation pattern, a frozen section examination is not reliable. PC is suspected if the mass is found to be large, hard, and lobulated; if it is in gray-white colour, and if a local invasion is observed in the operation 2,8. While parathyroid adenomas have a mean diameter of 1.5 cm, PC has a mean diameter of 3.4 cm. A pathological examination demonstrates local invasion, perineural invasion, and vascular invasion. Especially, the latter indicates malignancy. Malignancy is also suspected in the presence of capsular involvement, large fibrous bands, necrosis, a solid structure, increased mitosis, atypical mitosis, and nuclear atypia 1.7. The pathological examination makes the diagnosis of PC.
Adjuvant radiotherapy at a dose of 40-50 Gy can be given to patients if there is a high risk for local recurrences indicated by the presence of positive surgical margins, invasion or tumour rupture 8. It was reported that radiotherapy of the neck for postoperative or relapse may be beneficial for better local control 9. It was reported in the literature that recurrences were not observed over a period of 10 years in patients receiving radiotherapy 10. In case of metastatic disease and resistant hypercalcemia, chemotherapy may be used 8,10. Unfortunately, the efficacy of chemotherapy in parathyroid cancer has not been demonstrated in the literature 10. Our second patient received radiotherapy as tumour invasion into the thyroid tissue was observed in the pathological examination.
The most important prognostic factor in PC is to achieve a complete tumour resection. An extended tumour resection will improve the 5-year survival rates to 90% and 10-year survival rates to 67% 1. While local invasions occur most commonly in the ipsilateral thyroid gland and strap muscles, metastases are mostly observed in the lungs (40%), bones, and the liver 1,3. The risk of developing a local recurrence or distant metastasis ranges from 25 to 60% in five years 9-10. Morbidity and mortality usually occur due to refractory hypercalcemia and rarely due to tumour burden 1,10. The 5-year follow-ups of our patients were uneventful.
The morbidity and mortality of PC occur due to hypercalcemia rather than being due to the tumour itself. Hypercalcemia should be treated in patients with recurrences and metastases 10. Hypercalcemia crisis requires faster interventions with an aggressive saline infusion and administration of loop diuretics 1. Several modes of treatment were reported to be beneficial at variable rates, including treatment with bisphosphonates, calcimimetics, denosumab, mixamycin, plicamycin, calcitonin, glucocorticoids, and radiofrequency ablation 8,10. The efficacy of immunotherapy with the antiparathyroid hormone, and treatments with octreotide or azidothymidine are currently investigated 10.
Several biological markers were proposed to be used in the diagnosis and follow-up of the disease. High-risk patients can be identified with the use of CDC73 HRPT2 genetic mutation test. Parafibromin, Bcl-2a, and galectin-3 are the most useful adjunctive biomarkers. A low level of parafibromin has a prognostic value, indicating a poor prognosis and recurrences. In patients with low levels of parafibromin, genetic screening with CDC73/HRPT2 may contribute to the diagnostic processes 7,10.
In conclusion, the only chance to prolong the disease-free survival in PC is to perform an extended resection. A potential diagnosis of a parathyroid carcinoma should be considered in the presence of a large parathyroid gland, local invasion or regional lymph node involvement observed intraoperatively. In order to screen for PC and make the diagnosis, several biomarkers may be used including parafibromin, Bcl-2a, and galectin-3 and CDC73 / HRPT2 genetic testing can be performed.
References
- McClenaghan F, Qureshi YA. Parathyroid cancer. Gland Surgery. 2015;4:329-38.
- Basceken SI, et al. Is local resection sufficient for parathyroid carcinoma? Clinics. 2015;70:247?9.
- Sharretts JM, Kebebew E, Simonds WF. Parathyroid cancer. Semin Oncol. 2010;37:580-90.
- Wilkins BJ, Lewis JS. Non-functional parathyroid carcinoma:a review of the literature and report of a case requiring extensive surgery. Head Neck Pathol. 2009;3:140-9.
- Van der Zwan JM, et al. Carcinoma of endocrine organs: results of the RARECARE project. Eur J Cancer. 2012.48:1923-31.
- Hundahl SA, et al. Two hundred eighty-six cases of parathyroid carcinoma treated in the U.S. between 1985-1995: a National Cancer Data Base Report. The American College of Surgeons Commission on Cancer and the American Cancer Society. Cancer. 1999;86:538-44.
- Duan K, Mete Ö. Parathyroid Carcinoma: Diagnosis and Clinical Implications. Turk Patoloji Derg. 2015.31:1:80-97.
- Kolsi N, Jellali S, Koubaa J. Le carcinome parathyroïdien: à propos d?un cas et revue de la literature. Pan Afr Med J. 2017.27:85. French.
- Schulte K M, Talat N. Diagnosis and management of parathyroid cancer. Nat Rev Endocrinol. 2012.8:612-22.
- Betea D, Potorac I, Beckers A. Parathyroid carcinoma: Challenges in diagnosis and treatment. Ann Endocrinol (Paris). 2015;76:169-77.
|