Abstract
Fungus ball is a noninvasive, extramucosal mass of fungi usually characterized by a single sinus involvement. It is often asymptomatic, although it may cause non-specific symptoms such as headache, nasal obstruction, nasal discharge, etc. Fungus ball can also be seen in immunosuppressed patients. In literature, no sphenoid sinus fungus ball along with rheumatoid arthritis have been observed. In the light of current literature, this article discusses a patient with isolated sphenoid sinus fungus ball who has been on a long term treatment for rheumatoid arthritis and has severe headache complaint.
Keywords :
fungus
, sinusitis
, rheumatoid arthritis
Turkish Abstract
Fungus topu, ektramukozal yerleşimli invaziv olmayan ve genellikle tek bir sinüs tutulumu ile karakterize mantar enfeksiyonudur. Baş ağrısı, burun tıkanıklığı, geniz akıntısı gibi non-spesifik semptomlar verebilmesine rağmen çoğunlukla asemptomatik seyretmektedir. Fungus topu immunsüprese hastalarda da görülebilmektedir. Literatürde romatoid artrit ile beraber sfenoid sinüs mantar topu olgusuna rastlanılmamıştır. Bu makalede romatoid artrit nedeniyle uzun süredir tedavi gören ve şiddetli baş ağrısı şikayeti olan izole sfenoid sinüs fungus topu olgusu güncel literatür eşliğinde tartışılmıştır.
Turkish Keywords :
, mantar
, sinüzit
, romatoid artrit
Introduction
Fungal rhinosinusitis is histopathologically classified as invasive and non-invasive. Non-invasive fungal rhinosinusitis can be seen in immunosuppressed individuals and can be in the form of saprophytic fungal infestation, fungus ball or allergic fungal rhinosinusitis 1. Physiopathology formation of fungus ball is not clearly understood. According to a theory, the obstruction of sinus ostium and anaerobic infection and low pH value are effective in the development of fungus ball 2.
Fungus ball is usually asymptomatic, unilateral and non-invasive fungal infection with extramucosal location. It is primarily seen in the maxillary sinus, while it is seen in the sphenoid sinus secondarily. Isolated sphenoid sinus fungus ball accounts for approximately 10-15% of all cases 3. Due to the vital anatomic structures such as the skull base, optic nerve and carotid artery in the vicinity of the sphenoid sinus, the fungus collectors located in the sphenoid sinus are more serious and need more attention than the fungus collectors in the maxillary sinus 4.
Fungus ball is more common in immunosuppressed individuals with uncontrolled diabetes, cancer, rheumatologic disease and long-term steroid use. In literature, no fungus ball in the sphenoid sinus along with rheumatoid arthritis has been observed. In the light of current literature, this paper discusses a 55-year-old female patient with isolated sphenoid sinus fungus ball who has only severe headache complaint. The patient has been on a long-term treatment due to rheumatoid arthritis.
Case Report
A 55-year-old female patient with headache complaint was admitted to our outpatient clinic. It has been found out that the progressive headache has recently increased around the right eye and has not responded to analgesic treatment. It has been reported that the patient was diagnosed with rheumatoid arthritis about 20 years ago, does not have active symptoms and has been on methotrexate ( Koçak Farma; Tekirdağ; Türkiye) and salazoprine ( Pfizer; New York, ABD) treatment. There were no findings other than sedimentation and C-reactive protein (CRP) elevation in laboratory tests. Nasal endoscopic examination was natural except bilateral inferior concha hypertrophy. Paranasal sinus computed tomography (CT) examination showed soft tissue values ??suggesting a fungus ball in the right sphenoid sinus and filling the sinüs completely, having calcification in the centre but not causing destruction in bone structures (Figures 1-2).
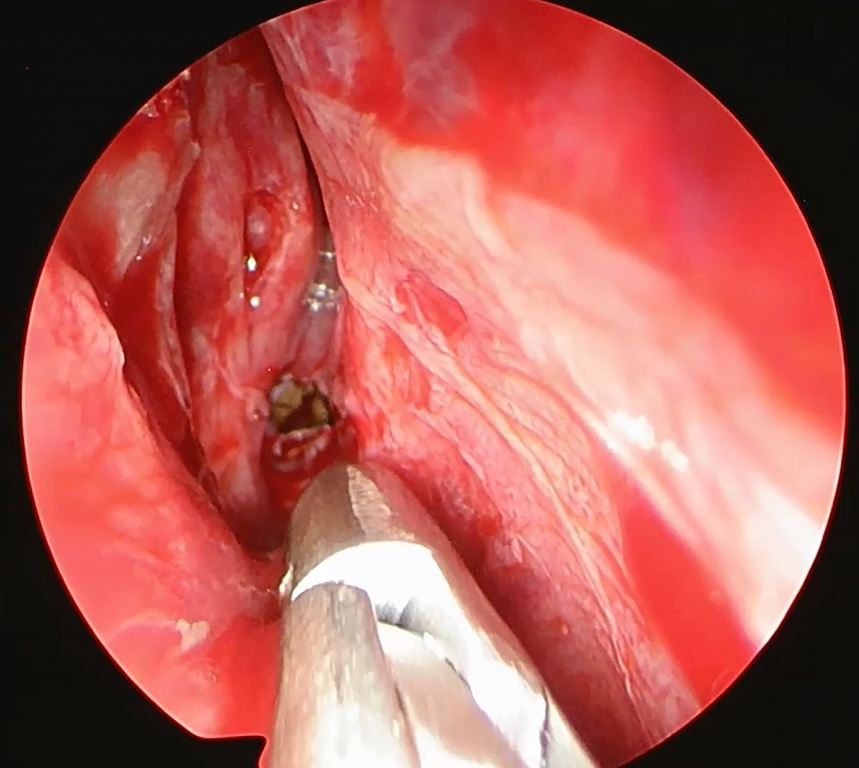
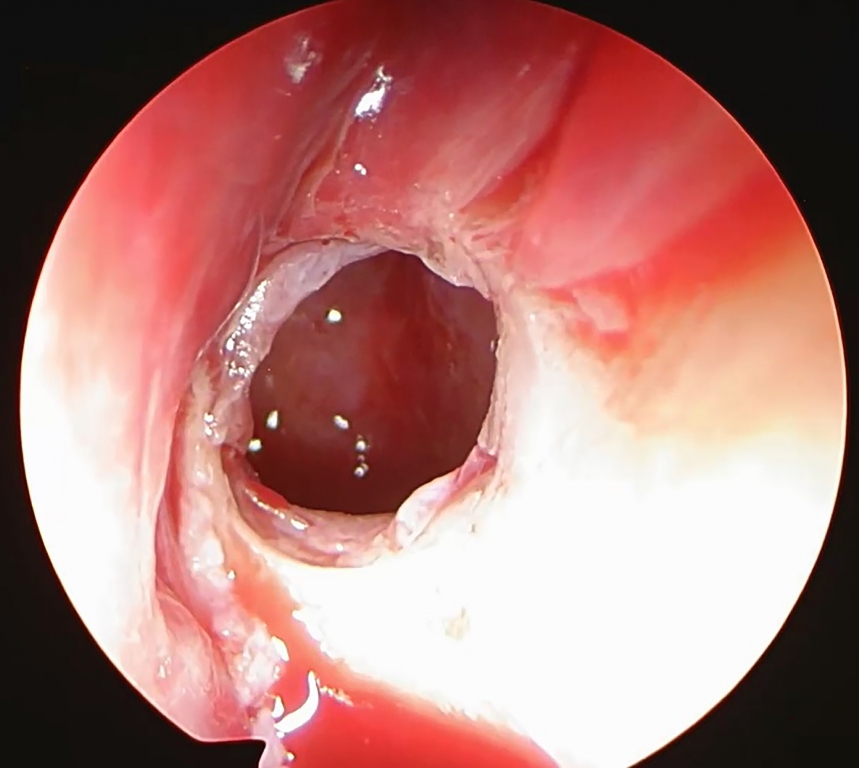
In the light of these findings, the patient was scheduled for right endoscopic sphenoidectomy based on the pre-diagnosis of a fungus ball in the sphenoid sinus. Superior concha was recognized and preserved through transnasal approach. Then, the sphenoid sinus ostium was found and enlarged. The fungus ball was removed from the sphenoid sinus then the sinus was cleaned and irrigated.(Figures 3-4).
The patient who did not develop any intraoperative or postoperative complications was found to have reduced complaints of headache after the operation. No recurrent symptoms and findings were found in the first postoperative month. Informed consent was obtained from the patient.
Discussion
The sphenoid sinus fungus ball is diagnosed in 5th-6th decades and is seen more frequently in females than males 5. Although, it is not a major cause of more frequent occurrence in women, hormonal factors have been shown to be relevant in some studies 3,6. While rhinological symptoms such as nasal obstruction, nasal discharge and smell impairment are common in the maxillary sinus-derived fungus ball; headache is seen more frequently in the sphenoid sinus around the eye. Our patient was a 55-year-old female patient and her only complaint was severe headache.
While immunosuppressive diseases play an important role in the development of invasive fungal sinusitis, immunosuppressive diseases are not at the forefront in the development of fungal ball. In their large series of studies by Lim HS et al., it was reported that the most common systemic disease in patients with isolated sphenoid sinus fungus was hypertension. In the same study, 10 patients was diagnosed with diabetes mellitus (DM), one patient with systemic lupus erythematosus (SLE) and one patient with thyroid cancer 5. Karkas et al. reported DM in 3 patients out of 28 cases with sphenoid sinus fungus ball, while no other immunosuppressive disease was identified 7. In literature, no isolated sphenoid sinus fungus ball along with rheumatoid arthritis have been observed. Our case is the first in literature in this respect. Our patient has been taking immunosuppressive treatment for about 20 years. She has a progressive headache that has appeared recently, we performed a CT examination and the disease was diagnosed in the paranasal sinus CT scan. Due to the fact that the fungus is usually asymptomatic, we cannot give a clear picture of for how long fungus ball has been present in our patient.
In the diagnosis of fungus ball, it is absolutely necessary to perform radiological evaluation before operation. Since, the sphenoid sinus is adjacent to the important anatomical structures, the presence of calcification and destruction in bone formation in the CT scan are important for the surgeon before the operation. Yoon YH et al., reported total fullness in 66% and partial fullness in 34% of the fungus balls. In the majority of cases, surface irregularities and calcifications in lesions were found. In addition, 56% had sclerosis in the sinus wall and 17.2% had bone erosion 8. Lim et al., found opacity that filled the sinus completely in 32 patients and partial opacity in 14 patients out of 46 cases with sphenoid sinus fungus ball. 69% of the cases were found to have opaque calcifications. Sclerosis in the sphenoid sinus walls and focal erosion in bone structures were noted in 69% of the patients 5. In our case, the patient had partial opacity in the sphenoid sinus and there were calcifications within the lesion. The anterior wall of the sphenoid sinus was seen as sclerotic at an advanced stage, which made it difficult to expand the sphenoid sinus ostium. No bone erosion in bone structures was observed in the CT examination. MRI imaging was not required as there was no intracranial or intraorbital complication in our patient.
As a surgical option, sphenoidectomy can be performed with transnasal or transethmoidal approach. If no pathology in the ethmoid sinus is present in the patient, the transnasal route is safer 9. In our case, sphenoidectomy was performed with transnasal route as there was no other nasal pathology except fungus ball in the isolated sphenoid sinus. Complications may occur during or after surgery. Apart from major complications such as optic nerve injury, carotid artery injury, minor complications such as hemorrhage and synechia can be seen especially postoperatively. No intraoperative or postoperative complications were observed in our patient. No recurrent symptoms and findings were found in the first postoperative month.
To conclude, it should not be forgotten that an isolated sphenoid sinus fungus ball may be present in a patient with rheumatoid arthritis who is suffering from chronic headache. Our case is a first in the literature in this respect.
References
- Chakrabarti A, et al. Fungal rhinosinusitis a categorization and de?nitional schema addressing current controversies. Laryngoscope. 2009;119:1809-18.
- Stammberger H. Endoscopic surgery for mycotic and chronic recurring sinusitis. Ann Otol Rhinol Laryngol. 1985;119:1-11.
- Nicolai P, et al. Fungus ball of the paranasal sinuses: experience in 160 patients treated with endoscopic surgery. Laryngoscope. 2009;119:2275-9.
- Bowman J, Panizza B, Gandhi M. Sphenoid sinus fungal balls. Ann Otol Rhinol Laryngol. 2007;116:514-9.
- Lim HS, et al. Isolated sphenoid sinus fungus ball: a retrospective study conducted at a tertiary care referral center in Korea. Eur Arch Otorhinolaryngol. 2017;274:2453-9.
- Klossek JM, et al. Functional endoscopic sinus surgery and 109 mycetomas of paranasal sinuses. Laryngoscope. 1997;107:112-7.
- Karkas A, et al. Sphenoid sinus fungus ball. Eur Arch Otorhinolaryngol. 2013;270:893-8.
- Yoon YH, et al. A retrospective analysis of 538 sinonasal fungus ball cases treated at a single tertiary medical center in Korea (1996-2015). Int Forum Allergy Rhinol. 2017;7:1070-5.
- Massoubre J, et al. Results of transnasal transostial sphenoidotomy in 79 cases of chronic sphenoid sinusitis. Eur Ann Otorhinolaryngol Head Neck Dis. 2016;133:231-6.
Information Presentation
Presented as a e-poster at the 14th Rhinology Congress, 28 April-1 May, 2018, Antalya, Turkey.
|