Abstract
Patients with extracranial carotid aneurysms may apply to Ear, Nose and Throat clinics with complaints of pulsatile mass in the neck, neurological symptoms or tinnitus. Glomus caroticum is one of the most common diagnoses of patients with a large mass of pulsatile neck. Herein, we present a case of common carotid artery aneurysm at the level of common carotid artery mimicking glomus caroticum. Glomus may coexist with an aneurysm in the carotid artery. Risk of complications during lesion excision may increase the presence of aneurysm. In patients admitted with a pulsatile mass lesion in the carotid bifurcation region, the diagnosis and treatment of aneurysm with glomus caroticum should be kept in mind.
Keywords :
Aneurysm
, Carotid body
, Glomus body
Turkish Abstract
Ekstrakranial karotis anevrizmaları olan hastalar, Kulak-Burun-Boğaz kliniklerine boyunda pulsatil kitle, tinnitus ve nörolojik semptomlarla başvurabilir. Boyunda kitle şikayeti ile başvuran hastalarda en sık görülen lezyonlardan biri glomus karotikumdur. Vaka takdimimizde, glomus karotikumu taklit eden common karotis arter bifurkasyon anevrizması sunulmuştur. Glomus karotis, arter bölgesinde anevrizma ile birlikte olabilir. Cerrahi olarak eksizyon esnasında anevrizma varlığında komplikasyonlarda artış olabilir. Boyunda pulsatil kitle lezyonu ile başvuran hastalarda tanı ve tedavi aşamasında glomus karotikum ve anevrizma akılda tutulmalıdır.
Turkish Keywords :
, Anevrizma
, Karotis Body
, Glomus Body
Introduction
Carotid artery aneurysm is a rare pathology of the head and neck. In the literature, carotid artery aneurysms are found in 1% of all aneurysms. Carotid artery aneurysms are approximately 4% of peripheral artery aneurysms 1. Carotid artery aneurysms can be divided into two, generally intracranial or extracranial. Carotid artery aneurysm can be divided according to the maintained carotid segment as the common carotid, external and internal carotid aneurysms. The internal carotid aneurysms are the most frequently reported aneuryms in the literature.
Patients with extracranial carotid aneurysms may apply to clinics with complaints of pulsatile mass in the neck, neurological symptoms or tinnitus. Glomus caroticum is one of the most common diagnoses of patients with a large pulsatile neck mass. Glomus caroticum is a rare tumor originating from paraganglionic cells. The location of glomus caroticum is the bifurcation of the carotid artery 2. Glomus caroticum, which can be seen simultaneously with aneurisms, has been reported in the literature 3. Aneurysm can be seen after resection of glomus caroticum.
Herein, we present a case of common carotid artery aneurysm at the level of common carotid artery mimicking glomus caroticum.
Case Report
A 38-year-old male patient was admitted to our hospital with a 1-year history of swelling in the left neck and with tinnitus complaints. The swelling in the neck region is observed in the left carotid bifurcation region. There was no history of trauma, diabetes mellitus, hypertension or any past medical history.
Physical examination revealed 2x1mm swelling in the left carotid bifurcation region. The lesion was palpable, fixed and not tender. The mass had a pulsation in the palpation. There was no pathology in the ear examination. Vital signs were normal. Audiological examination was in normal limits. No pathological findings were found in the patient's neurological examination. The patient's biochemical values, blood lipids, glucouse level were monitored at normal limits. Arterial blood pressure was monitored as 130/80.
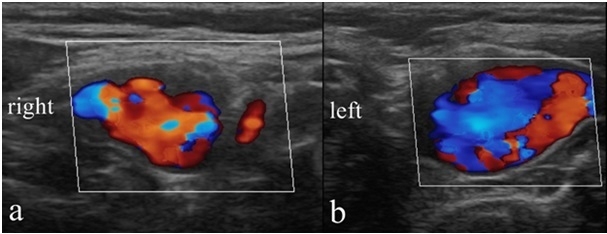
Investigations: Left common carotid artery bifurcation was asymmetrically wide according to the right, glomus caroticum and no other pathological findings were detected in neck ultrasonograhpy and Doppler ultrasonography (USG) ( Figure 1A, B).
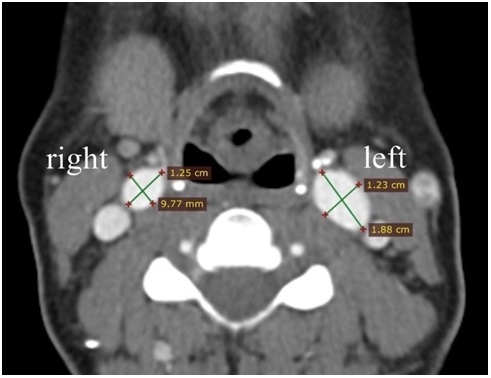
Contrasted tomography of the head and neck revealed a left right common carotid artery bifurcation with a diameter in the axial plane 9.7x12.5 mm, left commons carotid artery bifurcation with a diameter in the axial plane 12.3x18.8 mm, and left bifurcation diameter was asymmetrically greater than the width ( Figure 2).
Treatment and Follow up: The patient is consultated to Cardiovascular Surgery. The presence of cranial aneurysms was investigated by cranial magnetic resonance imaging (MRI) angiography. There was no pathology in MRI angiography. The patient was treated with anticoagulant theraphy initially. Operation and risks were explained to the patient. The patient was discharged because he did not accept the surgery.
The patient had given permission for the publication of this case report and the accompanying images.
Discussion
The carotid artery system moves to the base of the head after receiving the origin of the aorta. After giving bifurcation in the triangle of the neck, the external carotid artery moves externally. The internal carotid artery enters the cranial cavity from the base of the head. The carotid system is open to the development of aneurysms in the common carotid region, internal and external region.
Aneurysms that develop in the vascular system can be classified as real and false aneurysms 4. In the true aneurism (atherosclerotic aneurysm) is observed when the diameter of the vessel has expanded to over 50% as a whole. False aneurysm (pseudoaneurysm) is the enlargement of the artery wall that does not contain the full layers of the vessel, usually due to trauma or carotid dissection. True aneurysms can devolop from bifurcation or proximal internal carotid region 4. In an investigation from Mayo clinic 81% of aneurysms develop from internal carotid system, 11% from common carotid system and 8% from external carotid system 4.
Etiology differs whether the aneurysm is true or pseudoaneurysm. The main etiology of true aneurysms are mainly atherosclerosis, connective tissue disorders, inflammatory diseases, fibromuscular dysplasia and irradiation 5. The etiology of pseudoaneurysms is mainly trauma nad carotid aretry infection. Primary carotid artery infection may develop due to previous carotid surgery.
Aneurysms developed in extracranial carotid system were defined in the literature in 5 regions according to the location 6. According to this classification, type 1 is isolated internal carotid aneurysm, type 2 internal carotid aneurysm and bifurcation aneurysm, type 3 is only bifurcation aneurysm, type 4 internal and common carotid aneurysm, type 5 is isolated common carotid aneurysm. Our case was in accordance with type 3 extracranial aneurysms.
The symptoms of the disease depend on the location. Pulsatile mass lesion of bifurcation, neurological pressure symptoms, tinnitus, transitory ischemic attacks, serebrovascular events, ruptured complaints can be present in bifurcation lesions. A secondary infection may develop due to aneurysm.
Bifurcation localised aneurysms may interfere with carotid body paragangliomas. While aneurysm is fixed in palpation; glomus is defined as moving in the lateral direction but fixed in verticial direction 7. Imaging methods are important in the differential diagnosis. Glomus caroticum, which can be seen simultaneously with aneurism, has been reported in the literature 3 . Determining the current situation before the surgery is important in terms of reducing possible surgical complications.
The location, size, and symptoms of the aneurysm are important in the treatment of the disease. The patients with symptomathic extracranial carotid aneurysms, patients with thrombus in the lumen, above 2cm can be treated primarily with open and endovascular methods 8,9. In patients with asymptomatic cases below 2 cm, prophylactic anticoagulant therapy should be followed as it may be enlarged over time. The open surgical methods involve aneurysm excision and reconstruction, and carotid artery by pass 10,11. Endovasculary metal stent placement and embolization of the aneurysm sac, exclusion of the aneurysm using a stent-graft, or endovascular occlusion of the carotid artery methods can be used 12.
Conclusion
In patients admitted with a pulsatile mass lesion in the carotid bifurcation region, the diagnosis and treatment of aneurysm with glomus caroticum should be kept in mind 13. The risk of complications during the mass lesion in the glomus carotid may increase the presence of aneurysms 14. Proflactic treatment including anticoagulant theraphy should be initiated because of the risk of ischemia and serebrovasculary events. Development of carotid aneurysm may occur after glomus excision 15.
References
- Pourier VE, De Borst GJ. Which carotid artery aneurysms need to be treated (and how)? J Cardiovasc Surg (Torino). 2016 ;57(2):152-7.
- Ma D, et al. A retrospective study in management of carotid body tumour. Br J Oral Maxillofacial Surg. 2009;47:462-46.
- Mutlu V, Ogul H. Magnetic resonance imaging and magnetic resonance angiography findings of external carotid artery aneurysm and coexisting carotid body tumor. J Craniofac Surg. 2016 ;27(8):772-3.
- Fankhauser GT, et al. Surgical and medical management of extracranial carotid artery aneurysms. J Vasc Surg. 2015; 61:389-93.
- Reslan OM, Ebaugh JL, Raffetto JD. Bilateral asymptomatic extracranial carotid artery aneurysms. Ann Vasc Surg. 2010;24: 691;11-6.
- Attigah N, et al. Surgical therapy of extracranial carotid artery aneurysms: long-term results over a 24-year period. Eur J Vasc Endovasc Surg. 2009; 37:127-33.
- Al-Jarrah Q, et al. Surgical management of a symptomatic extracranial internal carotid artery aneurysm and coexisting carotid body tumor. J Vasc Surg Cases. 2015;1: 134-7.
- Pinzón M, et al. Endovascular management of iatrogenic cervical internal carotid artery pseudoaneurysm in a 9-year-old child: Case report and literature review. Int J Pediatr Otorhinolaryngol. 2017 95:29-33.
- Skóra JP, Kurcz J, Korta K, Szyber P, Dorobisz TA, Dorobisz AT. Surgical management of extracranial carotid artery aneurysms. Vasa. 2016;45(3):223-8.
- Matsukawa H, et al. Graft occlusion and graft size changes in complex ınternal carotid artery aneurysm treated by extracranial to ıntracranial bypass using high-flow grafts with therapeutic ınternal carotid artery occlusion. Neurosurgery. 2017 1;81(4):672-9.
- Maher CO, Meyer FB. Surgical treatment of nonatherosclerotic lesions of the extracranial carotid artery. Neurosurg Clin N Am. 2000 Apr;11(2):309-22.
- hong-ju bae, et al. Endovascular treatment of the distal ınternal carotid artery large aneurysm. J Cerebrovasc Endovasc Neurosurg. 2014 ; 16(3): 200-8.
- da Gama AD, et al. Displastic aneurysm of the internal carotid artery simulating a carotid body tumor Rev Port Cir Cardiotorac Vasc. 2009 ;16(3):179-80.
- Song AY, Myers EN, Gupta N. A case of mistaken identity: intraoperative discovery of an extracranial internal carotid artery aneurysm. Ann Vasc Surg. 2005 Nov;19(6):896-9.
- Hotze TE, Smith TA, Clagett GP. Carotid artery pseudo-pseudoaneurysm after excision of carotid body tumor. J Vasc Surg. 2011;54(3):864.
|