Abstract
Arachnoid cysts are fluid-filled sacs, that occur on the arachnoid membrane that covers the brain (intracranial) and the spinal cord (spinal) which are frequently detected incidentally during neuroimaging. Intracystic hemorrhage or subdural hematomas and subdural hygromas are rare complications of arachnoid cysts, typically occur after head trauma. In the literature there are a few cases of non-traumatic arachnoid cyst with complicating intracystic hemorrhage and bilateral subdural hematomas. In this report, we present a case of 42-year-old man with nontraumatic intracystic hemorrhage into a middle cranial fossa arachnoid cyst associated with a bilateral subacute subdural hematoma.
Keywords :
arachnoid cyst
, chronic subdural hematoma
, intracystic hemorrhage
Turkish Abstract
Araknoid kistler, sıklıkla santral sinir sistemi görüntülemelerinde rastlantısal olarak saptanan ve beyin (intrakranial) veya spinal kordu (spinal) çevreleyen araknoid membranlar üzerinde gelişen sıvı dolu keselerdir. Kist içi kanama veya subdural hematom ve subdural higromalar, araknoid kistin nadir komplikasyonları olup, tipik olarak travma sonrası meydana gelirler. Literatürde, kist içi kanama ve bilateral subdural hematom ile komplike, travmaya bağlı olmayan araknoid kist vakaları nadir görülmektedir. Bu yazımızda, 42 yaşında erkek hastada, herhangi bir travma ile ilişkisi olmayan orta kranial fossa yerleşimli araknoid kist rüptürüne bağlı olarak gelişen, kist içi kanama ve bilateral subdural hematom olgusunu sunuyoruz.
Turkish Keywords :
, Araknoid kist
, kist içi kanama
, subdural kanama
Introduction
Chronic subdural hematoma (SDH), has generally been believed to develop in elderly people several weeks after a head trauma 1. Also, in young people arachnoid cysts were identified as a cause of SDH after head trauma and are considered a risk factor for chronic SDH in this population 2. Arachnoid cysts with bilateral SDH in the absence of head injury are rare, and intracystic hemorrhage associated with SDH is even rarer 3.
In this report, we present computed tomography (CT) and magnetic resonance imaging (MRI) findings of a case of arachnoid cyst with spontaneous intracystic hemorrhage and a bilateral subdural hematoma.
Case Report
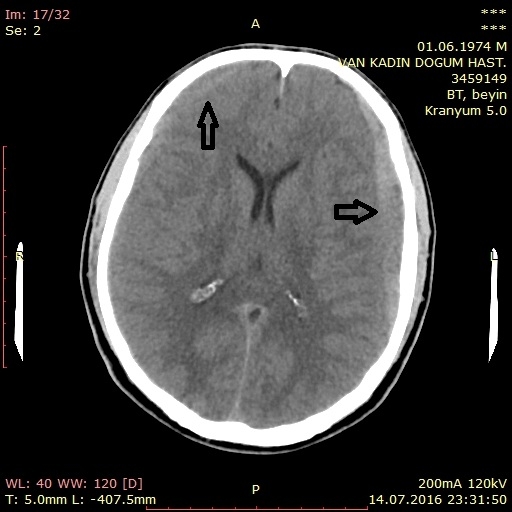
A 42-year-old male presented with a 5 day history of headache and nausea. There was no history of preceding head trauma and his medical history was unremarkable. A non-contrast head CT showed a hyperdense extra-axial collection consistent with a bilateral subdural hematoma. (Figure 1a).
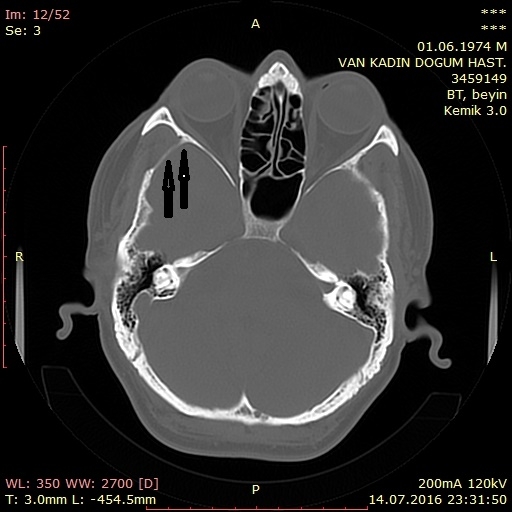
A lobulated mass-like appearance of extra-axial hemorrhage within the anterior aspect of the right middle cranial fossa was also noted (Figure 1b). There was also focal thinning with periosteal scalloping of both the squamous portion of the left temporal bone and of the adjacent greater wing of sphenoid bone (Figure 1c).
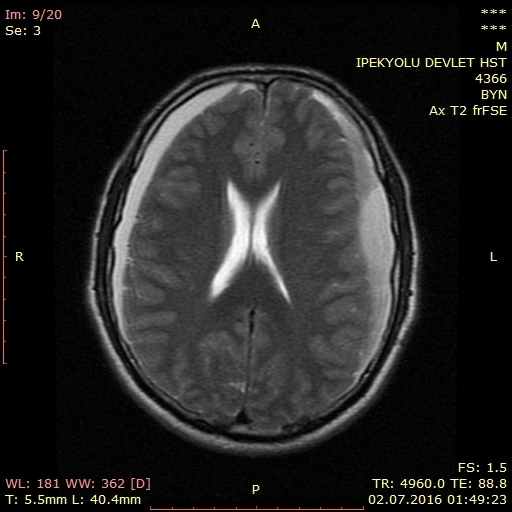
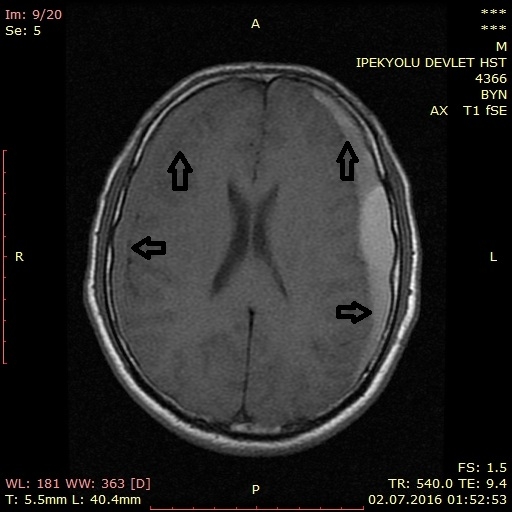
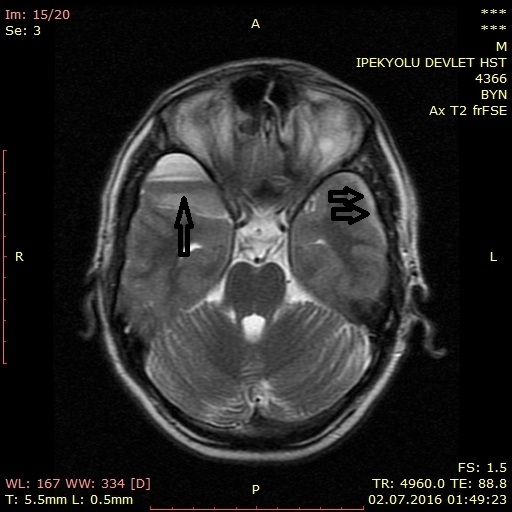
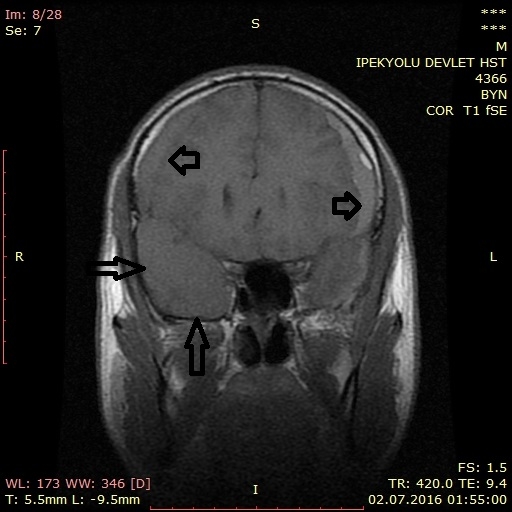
On T2-weighted MR imaging (Figure 2a) the subdural collection had a hyperintense signal to adjacent brain parenchyma while on T1-weighted MR imaging (Figure 2b) the collection demonstrated increased signal intensity. These findings were consistent with late subacute hemorrhage. Also on T2-weighted MR imaging hypointense bands consistent with hemosiderin deposits were also detected at the center of hemorrhagic cyst in the middle cranial fossa (Figure 2c,d).The hemorrhagic cyst was mildly hyperintense to adjacent brain parenchyma and bilateral subdural hematoma was hyperintense to adjacent brain parencyma on T1 weighted image.(Figure 2e)
With radiological findings, a diagnosis of intracystic hemorrhage and bilateral subdural hematoma secondary to arachnoid csyt rupture was made and a frontotemporal craniotomy with subdural hematoma evacuation and arachnoid cyst fenestration was performed.
Discussion
Arachnoid cysts constitute approximately 1% of all intracranial space-occupying lesions 4. The middle cranial fossa, cerebral convexity, perisellar, retrocerebellar, cerebellopontine angle, and quadrigeminal plate cisterns are the most common locations 5. It is believed that these cysts form from an aberration in arachnoid development which results in splitting or duplication of the membrane, from a defect in condensation of the mesenchyme, or from abnormalities of cerebrospinal fluid (CSF) flow 5,6.
Arachnoid cysts are non-enhancing, well-circumscribed extra-axial lesions with the same attenuation (on CT) or signal (on all MRI pulse sequences) as that of CSF on both CT and MRI scans 5. They do not communicate with the ventricular system and have no identifiable internal architecture. Bony erosion and remodeling, features suggestive of a longstanding process, are commonly associated with arachnoid cysts. These findings are seen in nearly half of the cases and are thought to be secondary to chronic fluid accumulation with transmitted pulsations 5,7.
Although, most arachnoid cysts are asymptomatic, symptoms may due to an increase of intracystic fluid or more rarely hemorrhage into the cyst itself and/or adjacent subdural space. Such hemorrhagic events may be commonly post-traumatic or rarely spontaneous. Rupture of the outer arachnoid cyst wall and surrounding fragile veins leads blood accumulation within the cyst and/or subdural compartment 8. Intracystic hemorrhage can also be due to interruption of the highly vascular arachnoid cyst membrane or of the bridging veins traversing the cyst cavity. Fluid production by flat arachnoid cells lining the cyst walls may explain spontaneous cyst enlargement and hemorrhage if sufficient intracystic pressure is attained to breech the wall and disrupt the vasculature 8.
Iaconetta et al., reviewed the literature that reported the very rare combination of intracystic bleeding with contralateral or bilateral subdural or extradural hematoma.They documented 37 such cases in the literature. In 21 cases (56.7%), there was ipsilateral subdural hematoma. Also, fourteen patients had a history of a previous head injury, whereas others did not 9.
Mori et al., reviewed twelve cases of subdural hematoma with arachnoid cyst which were surgically treated in their instution. Arachnoid cysts were located in the middle fossa (eight cases), convexity (two cases), and posterior fossa (two cases) in their patients. Ten of the 12 patients had a prior head trauma while two patients had spontaneous arachnoid cyst rupture leading to subdural hematoma. Five patients had right-sided, five patients had left-sided and two patients had bilateral subdural hematomas. Six of 12 patients had no radiologically demonstrated intracystic hematomas. All the radiologically demonstrated intracystic hematomas were demontrated on MRI. The most common clinical symptom was headache. Hematoma evacuation through burr holes improved the symptoms in all patients with arachnoid cyst 2.
Patel et al., presented CT and MRI features of a case with a spontaneous subdural hematoma and intracystic hemorrhage in an arachnoid cyst. They well demonstrated enhanced dural membrane, not enhanced arachnoid cyst and the arachnoid membrane which separates hemorrhage in the subdural compartment from hemorrhage inside the arachnoid cyst on contrast enhanced T1-weighted MR images 5.
Our patient also had a bilateral subdural hematoma which was associated with spontaneous arachnoid cyst hemorrhage. He had no head trauma or surgery history prior to presentation. He had a radiologically demonstrated intracystic hematoma on both CT and MRI. The low detection rates of intracytic hematoma on CT, can be attributed to the later phases of hematoma at the presentation. Also, hyperdense intracystic hematoma, relatively large and bilateral subdural hematoma which was seen in our patient may be secondary to an active bleeding.
References
- Markwalder TM. Chronic subdural hematomas: a review. J Neurosurg. 1981;54:637-45. [PubMed]
- Mori K, Yamamoto T, Horinaka N, Maeda M. Arachnoid cyst is a risk factor for chronic subdural hematoma in juveniles: twelve cases of chronic subdural hematoma associated with arachnoid cyst. J Neurotrauma. 2002;19:1017-27. [PubMed]
- Hong JC, Kim MS, Chang CH, Kim SH. Arachnoid cyst with spontaneous ıntracystic hemorrhage and chronic subdural hematoma. J Korean Neurosurg Soc. 2008 Jan; 43(1): 54-6.
- Osborn AG, Preece MT. Intracranial cysts: radiologic-pathologic correlation and imaging approach. Radiology. 2006 Jun;239(3):650-64. [PubMed]
- Patel AP, Oliverio PJ, Kurtom KH, Roberti F. Spontaneous subdural hematoma and ıntracystic hemorrhage in an arachnoid cyst. Radiol Case Rep. 2009; 4(3): 298.
- Gosalakkal JA. Intracranial arachnoid cysts in children: a review of pathogenesis, clinical features, and management. Pediatr Neurol. 2002 Feb;26(2):93-8. [PubMed]
- Parsch CS, et al. Arachnoid cysts associated with subdural hematomas and hygromas: analysis of 16 cases, long-term follow-up, and review of the literature. Neurosurgery. 1997 Mar;40(3):483-90. [PubMed]
- Huang D, et al. Intracystic hemorrhage of the middle fossa arachnoid cyst and subdural hematoma caused by ruptured middle cerebral artery aneurysm. Am J Neuroradiol. 1999; 20:1284-6. [PubMed]
- Iaconetta G, Esposito M, Maiuri F, Cappabianca P. Arachnoid cyst with intracystic haemorrhage and subdural haematoma: case report and literature review. Neurol Sci. 2006;26:451?455. [PubMed]
|