Abstract
This presented article reports a triad of left renal agenesis, ipsilateral seminal vesicle cyst and ejaculatory duct obstruction indicating Zinner syndrome in a 27-year old male with dysuria and infertility complaints. A review of the literature was also presented.
Keywords :
Zinner Syndrome
, Infertility
Turkish Abstract
Bu vakada disüri ve infertilite şikayetleri ile başvuran 27 yaşında erkek hastada tespit edilen agenetik böbrek, ipsilateral seminal vezikül kisti ve ejakulatör kanal obstrüksiyonunun birlikte olduğu bir triad olan Zinner Sendromunu literatür bulguları ile sunmayı amaçladık.
Turkish Keywords :
, Zinner Sendromu
, İnfertilite
Introduction
Zinner Syndrome is a rare congenital anomaly presenting with male infertility, unilateral renal agenesis, seminal vesicle cyst, and ipsilateral ejaculatory duct obstruction. Diagnosis is usually made at third or fourth decades.1,2 The case illustrated in this article is unique in terms of showing ultrasonograph (USG), intravenous pyelography (IVP), computed tomography (CT) urography and magnetic resonance imaging (MRI) urography findings alltogether.
Case Report
A-27-year old male admitted to the urology outpatient clinic with complaint of dysuria for one month. In urological anamnesis it was learnt that he was married five years ago and had been attempting to have a baby since two years. On physical examination external genitalia was normal and vasa deferentias were bilaterally palpable. On digital rectal examination prostate volume was normal and there was painful, smooth, bulky mass in the left prostatic region. Blood Urine Nitrogen, creatinine, Luteinizing Hormone, Follicule Stimulating Hormone, testosterone, prolactin in blood and urine test results were normal.
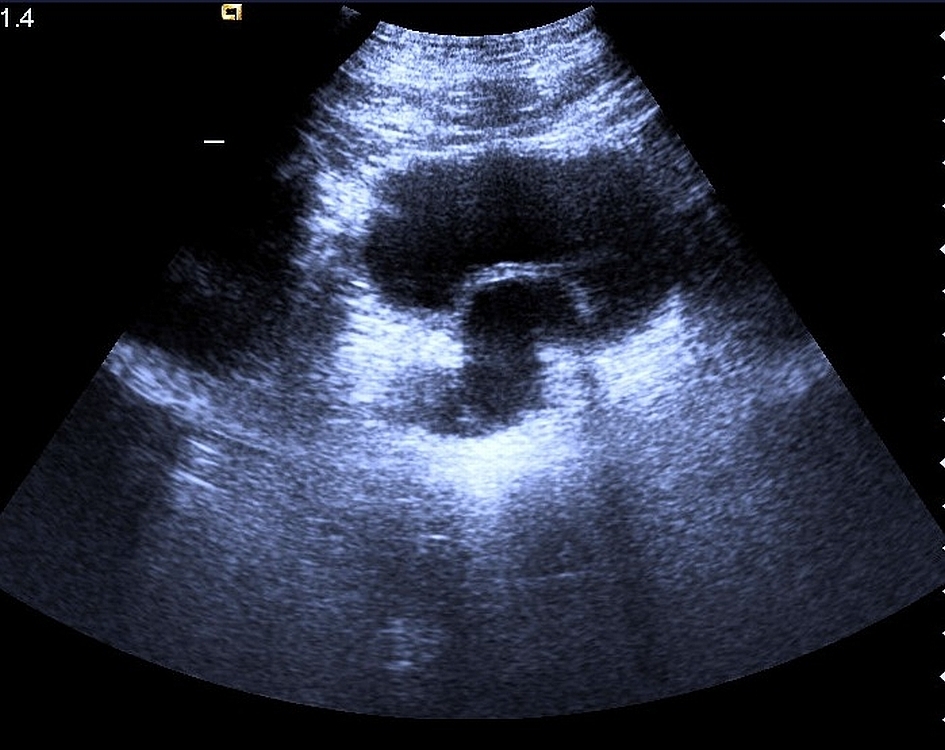
Radiological assessment consisted of transabdominal, pelvic, scrotal USG, scrotal color Doppler USG, IVP, CT urography and MRI urography. Transabdominal USG revealed a congenital agenesis of the left kidney with compensatory hypertrophy of the right kidney. A 32x24x22 mm sized cystic mass in the left seminal vesicle was detected (Figure 1).
Scrotal USG revealed a 12 mm sized left epididymal cyst and varicose veins at left side with maximum 3.7 mm diameter and moderate reflux indicating varicocele. On IVP no contrast enhancement was detected on left kidney location with hypertrophy in right kidney. There was also decompression effect at the left upper side of urinary bladder (Figure 2).
CT and MR urography were performed to determine the relationship of the cystic mass. On CT urography 43x23x25 mm sized cystic mass at place of left seminal vesicle and dilated vas deference were detected on left side (Figure 3).
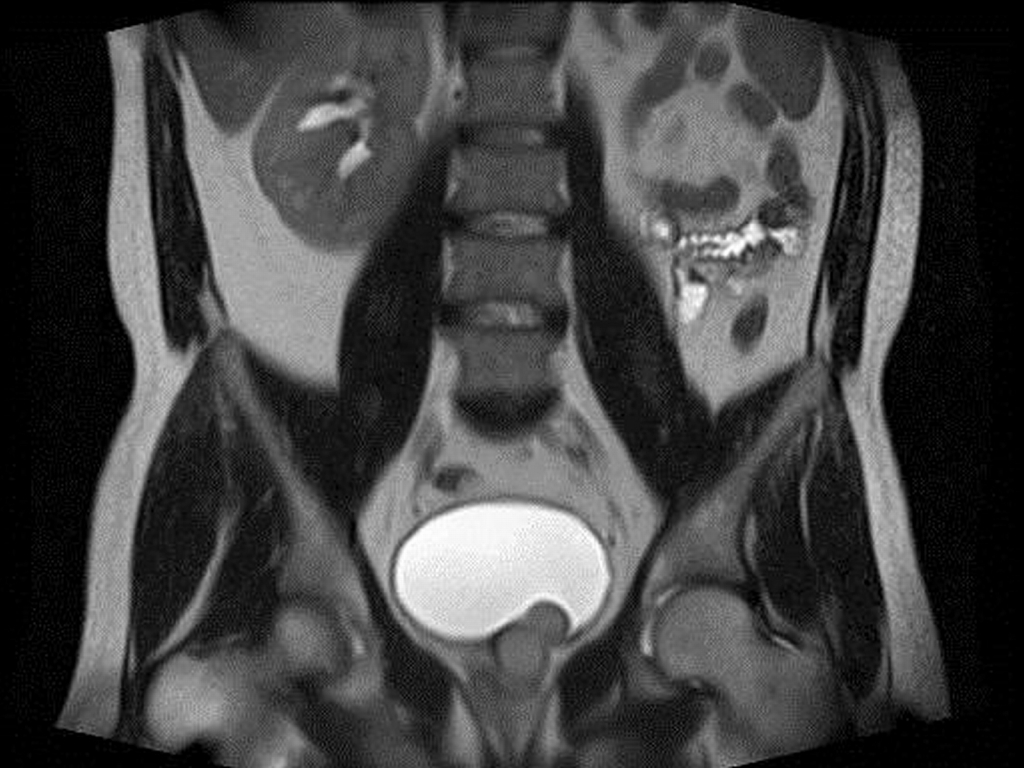
On MR urography cystic mass suggestive of haemorrhagic or proteinaceous content with hyperintensity on T1-WI (weighted images) and hypointensity on T2-WI was detected (Figures 4 and 5). There was agenesis of left kidney and left ureter.
Sperm volume was 1.7 cc, sperm count was 85.000.000 with 25% forward movements and 8% normal morphology indicating astenospermia. According to left sided renal agenesis, ipsilateral seminal vesicle cyst with ejaculatory duct obstruction the patient was diagnosed as Zinner syndrome. Laparoscopic seminal vesicle cyst excision was performed for treatment. In one month period control the result of sperm test was normal. Two months later we learned that his wife was pregnant.
Discussion
Zinner syndrome which was first reported in 1914 by Zinner is described as seminal vesicle cyst with ipsilateral renal agenesis 3. Since then fewer than 100 cases have been reported about the diagnosis and management of this rare syndrome. Absent ureter, existence of ureteral bud, absent trigone, testicular ectopia, contralateral seminal vesicle hypoplasia, adrenal gland malformation and vena cava malformation might be associated with this condition 3-5. Infertility is reported in 37.5% of cases.
Cysts of lower male genitourinary tract are rare and usually benign. These cysts may be associated with various congenital anomalies and they can be divided into two main groups according to location: intra-prostatic and extra-prostatic. Intra-prostatic cysts can be classified into median cysts, paramedian cysts and lateral cysts. Prostatic utricle cysts and Mullerian duct cysts are median cysts. Ejaculatory duct cysts are para-median cysts. Prostatic retention cysts, cystic degeneration of benign prostatic hypertrophy, cysts associated with tumors, and prostatic abscess are lateral cysts. Extra-prostatic cysts are the seminal vesicle, vas deferens, and Cowper duct cysts 6. Other lesions like ureterocele, defect resulting from transurethral resection of the prostate gland, bladder diverticulum, hydroureter and ectopic insertion of ureter might mimic these cystic lesions.
Seminal vesicle cyst is a rare entity. It may be congenital or acquired due to obstruction and inflammation 6,7. Seminal vesicle cysts might be associated with upper urinary tract anomalies and autosomal dominant polycystic kidney disease8. Diagnosis is usually made in 3rd or 4th decade which usually develops during the years of sexual activity due to inadequate drainage of secretions but might be detected earlier due to increasing use of imaging modalities 9. Patients with seminal vesicle cysts may be asymptomatic or have symptoms of chronic recurrent prostatitis, recurrent epididymitis, painful ejaculation, urethral discharge, urgency, hesitancy, hematuria, acute urinary retention, pain upon defecation, tenesmus, constipation, pelvic discomfort, perineal or testicular pain, an abdominal or pelvic mass, infertility, or hematospermia. Generally cysts <5cm are asymptomatic and large cysts (>8-10cm) are symptomatic. Other cystic lesions like ureterocele, Mullarian duct cysts and prostatic cysts might mimic seminal vesicle cysts 6,10,11. The main distinguishing factor of seminal vesicle cyst is the association with other congenital anomalies of genitourinary tract. Ureterocele is a saccular lesion of distal end of the ureter. The position of ureterocele is where the ureter would have inserted and it is usually unilateral. It may be asyptomatic or symptoms of dysuria, urgency, and recurrent urinary infections may present. On CT and USG round mass inside the bladder is detected 6. Mullarian duct cysts occur above the base of prostate in the midline. These cysts result from inadequate regression of mesonephric duct. Association with upper urinary tract anomalies is detected only in 10% of the cases. The distinguishing factors of Mullarian duct cysts are the median location and not to containing spermatozoa but commonly containing calculi 12. Prostatic cysts can be either midline or lateral location and usually smaller (0.75-3cm) 11. Prostatic cysts are usually simple cysts with thin wall and are unilocular.
More commonly the diagnosis is made by IVP, USG and cross sectional imagining modalities like CT and MRI. In one case of non-Hodking?s lymphoma cystic mass within the bladder was detected in positron emission tomography incidentally and after confirmation with CT urography the diagnosed was made 7.
On IVP renal and ureteral agenesis and filling defect within bladder might be detected. On USG anechoic mass within the seminal vesicle, larger anechoic saccular lesion, which may arise from the pelvis and displace the bladder and other pelvic structures might be manifested. USG can be used for drainage by needle and to delineate the lesion more fully in combination with contrast injection 9,13. However, vasovesiculography (aspiration of the cyst and injection of contrast agent) is rarely done to avoid complications in symptomatic patients 10. Density on CT and signal intensity on MRI is based on the protein content or hemorrhage within the cyst. Generally due to high protein content cysts have high density on CT. On MRI variable signal on T1 and T2 weighted images might be detected due to hemorrhage or proteinaceous fluid.
Neoplasia of epithelium can occur in seminal vesicle cysts that may cause symptoms after surrounding the other pelvic structures, making excision at this stage as a morbid procedure. Thus, although seminal vesicle cysts are generally in benign nature, early removal could prevent the development of symptoms and neoplasia 14. Open and minimally invasive procedures (laparoscopic or robotic excision) are the treatment of choice in patients 15. When compared with robotic and laparoscopic surgery, robotic procedures have been shown to be associated with less blood loss, quick convalescence and minimal pain 15.
In conclusion, various types of cysts can affect the lower male genitourinary tract. These lesions may be found incidentally at imaging or may manifest symptoms such as hematuria, dysuria, hematospermia, urinary incontinence or infertility. It is important to be aware of and consider alternative imaging modalities for diagnosis. Differentiation can be made on the basis of location, contents and association with renal or genital anomalies. Minimally invasive procedures can be preferred for treatment in early stage.
References
- Livingston L, Larsen CR. Seminal vesicle cyst with ipsilateral renal agenesis. AJR Am J Roentgenol. 2000; 175(1):177-80.
- Gianna P, Giuseppe PG, Carlo V. Mayer-Rokitansky-Küster-Hauser syndrome and the Zinner syndrome, female and male malformation of reproductive system: Are two separate entities. J Chinese Clin Med. 2007; 2:11.
- Cherullo EE, et al. Laparoscopic management of congenital seminal vesicle cysts associated with ipsilateral renal agenesis. J Urol. 2002; 167(3):1263-7.
- Kyriakidis A, et al. Zinner's syndrome associated with adrenal gland and vena cava malformation: a very rare case. Br J Urol. 1995; 76(4):523-4.
- Kardoust Parizi M, Shakhssalim N. Management of Zinner's Syndrome Associated with Contralateral Seminal Vesicle Hypoplasia: A Case Report. Case Rep Urol. 2013; 2013:494215.
- Shebel HM, et al. Cysts of the lower male genitourinary tract: embryologic and anatomic considerations and differential diagnosis. Radiographics. 2013; 33(4):1125-43.
- Kuo J, Foster C, Shelton DK. Zinner's Syndrome. World J Nucl Med. 2011; 10(1):20-2.
- Arora SS, et al. CT and MRI of congenital anomalies of the seminal vesicles. AJR Am J Roentgenol. 2007; 189(1):130-5.
- Steers WD, Corriere JN Jr. Case profile: seminal vesicle cyst. Urology. 1986; 27(2):177-8.
- Van den Ouden D, et al. Diagnosis and management of seminal vesicle cysts associated with ipsilateral renal agenesis: a pooled analysis of 52 cases. Eur Urol. 1998; 33(5):433-40.
- Gevenois PA, et al. Cysts of the prostate and seminal vesicles: MR imaging findings in 11 cases. AJR Am J Roentgenol. 1990; 155(5):1021-4.
- Curran S, et al. Endorectal MRI of prostatic and periprostatic cystic lesions and their mimics. AJR Am J Roentgenol. 2007; 188(5):1373-9.
- Shabsigh R, et al. The role of transrectal ultrasonography in the diagnosis and management of prostatic and seminal vesicle cysts. J Urol. 1989; 141(5):1206-9.
- Lee BH, et al. Primary mucinous adenocarcinoma of a seminal vesicle cyst associated with ectopic ureter and ipsilateral renal agenesis: a case report. Korean J Radiol. 2007; 8(3):258-61.
- Sridhar A, et al. Robot-assisted management of Zinner?s syndrome: report of seminal vesicle sparing technique and review of literature. Journal of Robotic Surgery. 2014; 8(2):185-7.
|