Abstract
Hand, foot and mouth disease (HFMD) is a highly infectious childhood disease and mostly caused by Coxsackievirus A16 and Enterovirus 71. It is a benign, self-limiting disease and characterized by mild clinical symptoms including fever with typical erythematous papules on the hands, feet, and oral cavity. This disease is rarely seen in healthy adults.
A 39-year-old Turkish male applied with fever, sore throat, malaise and multiple vesicles on both palms and soles. His 5-year-old son had same symptoms and had been diagnosed with HFMD 7 days ago. The patient was diagnosed with HFMD based on history, characteristic skin lesions and Polymerase chain reaction (PCR) analysis and was treated symptomatically. The lesions resolved spontaneously in 10 days without any complications during a 5-month follow-up.
In this report, we describe a case of HFMD caused by Coxsackievirus A16 in an immunocompetent adult. Although, HFMD is rarely seen in healthy adults, the disease should always be kept in mind in patients who present with fever, malaise and maculopapular rashes.
Keywords :
Hand-foot and mouth disease
, Coxsackievirus A16
, Enterovirus 71
Turkish Abstract
El-ayak-ağız hastalığı, çoğunlukla Koksakivirus A16 ve Enterovirus 71?in neden olduğu, oldukça bulaşıcı bir çocukluk çağı hastalığıdır. Eller, ayaklar ve oral kavitede görülen eritamatöz papüller döküntüler ile ateşin olduğu hafif klinik semptomlarla seyreden ve kendini sınırlayan bir hastalıktır. Bu hastalık sağlıklı erişkinlerde nadir görülür.
Otuzdokuz yaşında erkek hasta ateş, boğaz ağrısı, halsizlik ve her iki avuç içi ile ayak tabanında çok sayıda veziküler döküntü şikayeti ile başvurdu. Aynı şikayetleri olan 5 yaşındaki oğluna bir hafta önce el-ayak-ağız hastalığı tanısı konulmuştur. Hasta, hikayesi, karakteristik deri lezyonları ve polimeraz zincir reaksiyonu (PZR) analizi sonucu el-ayak-ağız hastalığı tanısı aldı ve semptomatik olarak tedavi edildi. Lezyonlar 10 gün içinde kendiliğinden söndü ve 15 aylık takibinde komplikasyon gözlenmedi.
Bu bildiride, immunkompetan bir yetişkinde Koksakivirus A16?nın neden olduğu bir el-ayak-ağız hastalığı vakasını tanımladık. El-ayak-ağız hastalığı sağlıklı yetişkinlerde az görülmesine rağmen ateş, halsizlik ve makulopapüler döküntüler ile başvuranlarda bu hastalık akılda tutulmalıdır.
Turkish Keywords :
, El-ayak-ağız hastalığı
, Koksakivirus A16
, Enterovirus 71
Introduction
Hand, foot and mouth disease (HFMD) is a highly contagious disease and mostly caused by Coxsackievirus A16. HFMD can also be caused by Coxsackieviruses A5, A7, A9, A10, B2, B5, and Enterovirus 71. HFMD is predominantly a childhood disease seen in summer 1. The disease is characterized by mild prodromal symptoms including fever, sore throat and malaise. This onset is usually followed by vesicular exanthema on the palms and feet 2. The lesions and the other symptoms resolve within 7 to 10 days 3. In the present paper, we report HFMD in a healthy adult.
Case Report
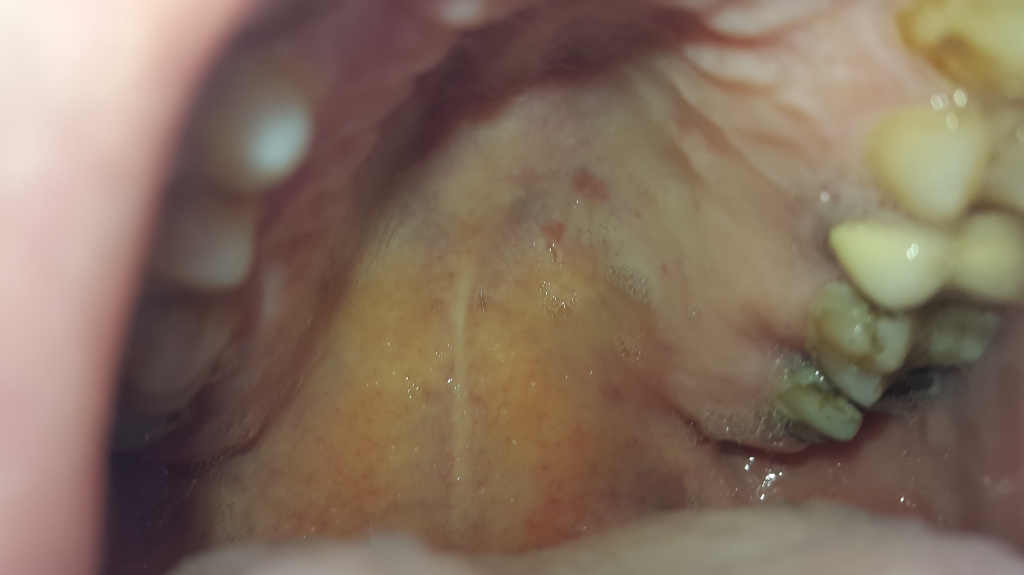
In November 2014, A 39-year-old Turkish male was admitted to our clinic with fever, sore throat, malaise and multiple vesicles on both palms and soles for a period of three days. He had good past health and was not taking medications. He had no recent travel history. Seven days ago, his 5-year-old son had same symptoms and had been diagnosed with HFMD. On physical examination, he was noted to have oral mucosal lesions (Figure 1), multiple erythematous papules and vesicles on his palms and soles (Figure 2, Figure 3).
Complete blood count revealed no abnormalities. The erythrocyte sedimentation rate was 20 mm/h. Blood chemistry tests showed mildly elevated transaminases (AST: 64?U/L, ALT: 100?U/L) and an elevated CRP level (55 mg/l). Serology for Syphilis, HIV, Cytomegalo-virus, Epstein-Barr virus, Measles and Rubella were negative. The electrocardiogram, echocardiogram and chest X-ray findings were unremarkable. Polymerase chain reaction (PCR) of the sample aspirated from a skin lesion and a swab taken from a nasopharyngeal lesion were positive for coxsackievirus A16. The patient was diagnosed with HFMD based on history, characteristic skin lesions and PCR analysis. The patient was treated symptomatically and the lesions resolved spontaneously in 10 days without any complications during a 5-month follow-up.
Discussion
Hand, foot and mouth disease is an acute, common, highly infectious viral disease that mainly affects preschool children in summer. It is a benign, self-limiting disease. However, in a minority of the cases, severe form can be seen in children and adults caused by uncommon types of the virus. The infection is characterized by mild clinical symptoms including fever with typical erythematous papules on the hands, feet and oral cavity, but it is usually asymptomatic 4. Most of the cases recover completely within 1 week 5.
Several enteroviruses can cause HFMD, but it has been mainly associated with Coxsackievirus A16 and Enterovirus 71 6. In children, HFMD caused by Enterovirus 71 has higher complication rates than Coxsackievirus A16 infection, like brainstem encephalomyelitis, neurogenic pulmonary edema, pulmonary hemorrhage, shock, and rapid death. However, Coxsackievirus A16 can also cause myocarditis, pericarditis, and shock 7. Cases are usually diagnosed according to clinical presentation. Serology, PCR and viral culture can also be used for an accurate diagnosis 6,8.
Hand, foot and mouth disease is usually treated symptomatically. HFMD mostly affects children and immunocompromised adults. Elderly people and pregnant women are also susceptible to HFMD. Immunocompetent adults are rarely affected, but recently, HFMD cases have been reported in the literature in healty adults 4,9-12. Disease is transmitted by oral-oral, fecal-oral and/or respiratory routes among family members 9.
In this present paper, we describe an healty adult with HFMD. His 5-year-old son had same symptoms and had been diagnosed with HFMD clinically 7 days ago. Diagnosis of HFMD was made based on family history, typical clinical and cutaneous features. The causative agent was comfirmed as Coxsackievirus A16 by PCR testing.
Clinical course of HFMD is usually benign. Rarely, serious complications, especially in small children, the elderly, pregnant or immunocompromised people such as cardiomyositis, aseptic meningitis, pneumonia can be seen. Though, a rare entity in immunocompetent adults, clinicians must take HFMD into consideration as a differential diagnosis in unclear cases with fever and skin lesions. Since HFMD is highly contagious, the patients in risk categories may develop severe complications. Therefore, early diagnosis, isolation and hygienic precautions are very important and essential to prevent spreading of the disease to vulnerable groups.
References
- Robinson CR, Doane FW, Rhodes AJ. Report of an outbreak of febrile illness with pharyngeal lesions and exanthem: Toronto, summer 1957; isolation of group A Coxsackie virus. Can Med Assoc J 1958; 79: 615-21.
- Miller GD, Tindall JP. Hand-foot-and-mouth disease. JAMA 1968; 203: 827?30.
- Flett K et al. Hand, foot, and mouth disease caused by coxsackievirus A6. Emerg Infect Dis 2012; 18: 1702-4.
- Centers for Disease Control and Prevention (CDC). Notes from the field: severe hand, foot, and mouth disease associated with coxsackievirus A6?Alabama, Connecticut, California, and Nevada, November 2011-February 2012. MMWR Morb Mortal Wkly Rep 2012; 61: 213-4.
- Wang Q et al. Clinical features of severe cases of hand, foot and mouth disease with EV71 virus infection in China. Arch Med Sci 2014; 10: 510?6.
- Osterback R et al. Coxsackievirus A6 and hand, foot and mouth disease. Emerg Infect Dis 2009; 15: 1485-8.
- Abzug MJ. Nonpolio Enteroviruses. In : Kliegman RM, Stanton BF, Geme JW, Schor NF, Behrman RE eds. Nelson Textbook of Pediatrics, 19th Edition. Philadelphia: Elsevier, 2011 pp:1090.
- Tsao KC et al. Use of molecular assay in diagnosis of hand, foot and mouth disease caused by enterovirus 71 or coxsackievirus A 16. J Virol Methods 2002; 102: 9-14.
- Shin JU, Oh SH, Lee JH. A case of hand-foot-mouth disease in an immunocompetent adult. Ann Dermatol 2010 ;22: 216-8.
- Shea YF et al. Hand, foot and mouth disease in an immunocompetent adult due to Coxsackievirus A6. Hong Kong Med J 2013; 19: 262?4.
- De Lima BF et al. Hand, foot, and mouth syndrome in an immunocompetent adult: a case report. BMC Research Notes 2013; 6: 441.
- Akkoyunlu Y, Ceylan B, Aslan T. Hand, foot, and mouth disease in an adult. Braz J Infect Dis 2014; 18: 227?8.
Information Presentation
This article has been presented as poster in the 2. International Emergency Medicine Congress, Rixos Sungate Hotel, Antalya, 15-19 April 2015
|