Abstract
Laparoscopic Roux-en-Y gastric bypass (LRYGB) is being increasingly performed for obesity. Internal herniation is one of the most important LRYGBP surgery complication seen 0.2?5% of the cases.In 9.1% of the cases the herniation will lead to ischemia and perforation, with a mortality rate of 1.6%.The rapid weight loss in the child baring age woman leads to; the increase in libido and fertility thus increasing the chance of a pregnancy cases. With the internal herniation leading to ischemia and perforation, maternal and fetal mortalities are reported in the literature. Here we present a case of maternal and fetal death due to internal herniation after LRYGB surgery.
Keywords :
Obesity surgery
, Pregnancy
, Laparoscopic bypass
, Internal herniation
, Fetal death
, Mortality
, Short bowel syndrome
Turkish Abstract
Laparoskopik Roux-en-Y gastrik bypass (LRYGB), obezite cerrahisinde sıklıkla uygulanan bir tekniktir. Internal herniasyon bu cerrahinin %0,2-%5 oranında görülen en önemli komplikasyonlarındandır. Bu vakaların %9.1?sinde bu herniasyon, iskemi ve perforasyona neden olur, bu durumun mortalitesi ise %1,6?dir. Hızlı kilo verilmesi, çocuk doğurma yaşında olan kadınlarda, libidoyu ve üretkenliği yükseltip, gebe kalma ihtimalini arttırmaktadır. Internal herniasyon sonucunda iskemi ve perforasyon nedeni ile görülebilen feto-maternal kayıplar literatürde bulunmaktadır. Biz burada, LRYGB sonucunda oluşan internal herniasyona bağlı anne ve bebek kaybı ile sonlanan bir vakayı sunduk.
Turkish Keywords :
, Obezite cerrahisi
, Gebelik
, Laparoskopik bypass
, İnternal herniasyon
, Fetal kayıp
, Mortalite
, Kısa barsak
Introduction
In fertile women, laparoscopic Roux-en-Y gastric bypass (LRYGB) is being increasingly performed for obesity. Internal herniation is one of the most important LRYGBP surgery complication seen 0.2?5% of the cases 1. Especially seen in pregnancies after bariatric surgery due to high intra-abdominal pressures leading to intestinal loop herniation . In 9.1% of the cases the herniation will lead to ischemia and perforation, with a mortality rate of 1.6% 2. Maternal and fetal mortalities are reported.
Case Report
Here we present a 16 weeks pregnant 42-year-old woman with a history of LRYGB performed three years ago. During these 3 years after the surgery, she has lost over 50 kg.
She presented to the emergency department with acute onset of an abdominal pain and nausea, vomiting. The abdominal examination demonstrated diffuse pain, worst on the left side, with associated guarding, rebound, and abdominal rigidity. There was a hemorrhagic fluid in the aspirate from the naso-gastric drain inserted. After the obstretrics and gynecology examination a normal living intrauterine pregnancy was approved. Her laboratory findings supported the clinical and physical findings of the acute abdomen. With physical examination and laboratory findings, she was taken to the operating room for an exploratory laparotomy.
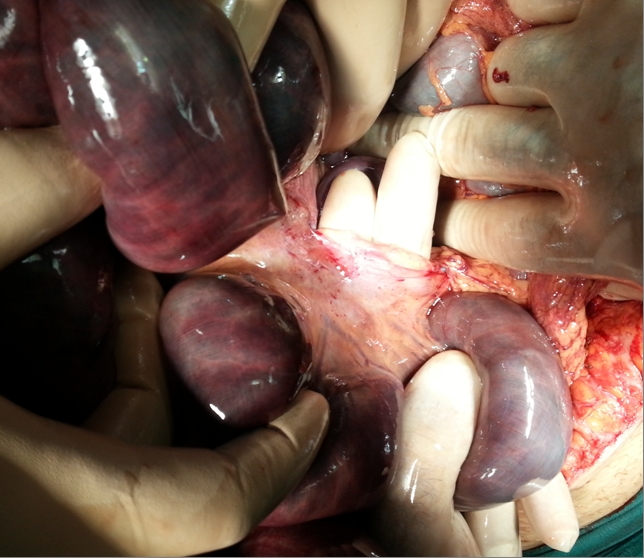
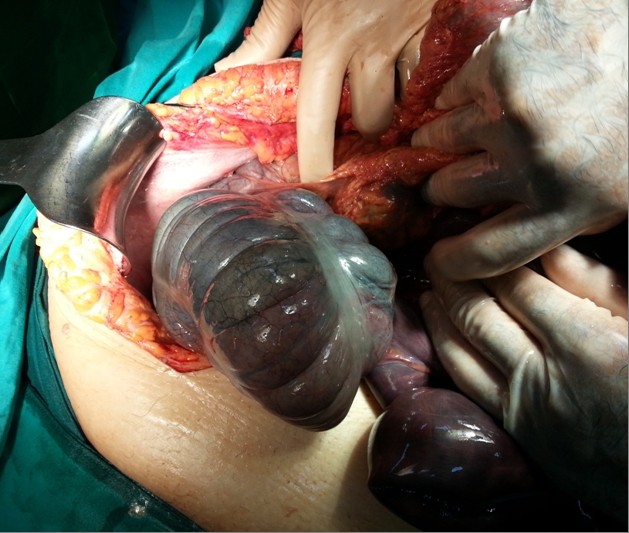
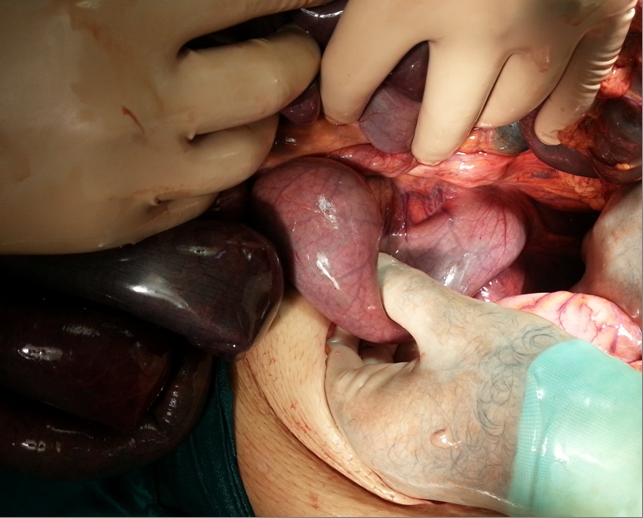
In the laparatomy an internal herniation and a strangulation of a small bowel segments starting from the jejunum up to the middle of the transverse colon was seen (Figures 1,2,3,4).
All these internal herniated bowel segments were necrotic but the gastric remnant was vital. Extended small bowel resection and a right hemicolectomy were performed. After the bowel resection only a 40 cm of jejunum was left in place (Figure 5). Intra-operative obstetric consultation was done and there were no fetal heart beat and the pregnancy was terminated.
The gastric roux-en-Y anastomosis was stapled and closed in the operation. End-jejunostomy was done and she was hospitalized with a 24 hours of naso-gastric decompression because the intestinal passage was interrupted and parenteral nutrition was given because of the short bowel syndrome.
After 2 weeks, she was taken to the operating room to establish the continuity of the digestive system and the staple closed gastric anastomosis was redone by a gastro-gastrostomy. The jejuno-colonic anastomosis was performed. She was discharged from the hospital with a moderate oral intake and a parenteral nutrition support. Because of the short bowel syndrome she had a small bowel transplantation in another center after 6 months from the initial surgery. But she died due to the complications of the small bowel transplantation.
Discussion
Body mass index (BMI) ?40 is the criteria for morbid obesity. Currently surgery offers the only treatment option with good long-term results in obese patients that could not lose weight and/or keep their normal weight. Laparoscopic Roux-en-Y gastric bypass (LRYGBP) is the most common bariatric surgical procedure performed for morbid obesity in young women .
The rapid weight loss in the child baring age woman leads to; the increase in libido and fertility thus increasing the chance of a pregnancy 3 .Pregnancy especially 12-18 months after the LRYGBP surgery is shown to be safe in the follow-up of LRYGBP operated woman 4. Other then the common risks of the laparoscopic surgery like bleeding, anastomosis leak, infection etc. LRYGBP surgery?s most common and important complication is the internal herniation with a risk of 0.2?5% 1. The pathogenesis of this internal herniation is thought to be due to the limited exposure and the control of the mesentery in the laparoscopy, the iatrogenic defects of mesentery caused by the surgery. Also after the surgery due to the loss of intra-abdominal fat, the enlargement of the defects that maybe small at the time of the operation are other potential pitfalls 5. Internal herniation is generally seen around 1 year after the surgery. In 9.1% of the cases the herniation will lead to an ischemia of the strangulated and incarcerated intestinal segment leading to intestinal perforation, with a mortality rate of 1.6% 2.
When the pregnancy is encountered there are also maternal and fetal mortality reports in the literature due to the internal herniation after LRYGB surgeries 6. Maternal death occurred in 2 cases (9%) and fetal death in 3 (13.6%) in reviews 7.
The potential anatomical defects that are created in the LRYGBP surgery changes in number due to the alimentary roux-limb positioning chosen in the surgical technique by the surgeon. If the limb is positioned retro-colically than the Internal herniation may occur in; the Petersen?s space , the transverse mesocolon defect and the jejuno-jejunostomy mesenteric defect. But if the same alimentary roux-limb is positioned ante-colically than only two potential spaces; the Petersen?s space and the jejuno-jejunostomy mesenteric spaces may become a potential sites for the internal herniation 8.
Dealing with pregnant patients is a major problem in surgical practice. Because the radiation dose used in the abdominopelvic CT is generally below the threshold of the dose for a fetal damage, in scenarios where immediate intervention is needed and early diagnosis is vital, CT can be used 9. But in cases with high suspicion direct laparatomy/laparoscopy should be performed in the first place without losing any more time. In our patient, the diagnosis of intestinal infarction due to internal hernia was suspected by clinical findings and CT, confirmed by operation.
Conclusion
As the obesity and obesity related diseases are growing in number. The bariatric surgeries will be performing more and more common. Like the gastric bypass surgeries the laparoscopic upper GI surgeries must be kept in mind for similar complications. Even for surgeons not dealing with the bariatric surgical interventions; young patients who have had a LRYGBP surgery over a year and especially the pregnant patients with abdominal pain must bring out the suspicion of an internal herniation.
Recurrent Emergency Room admissions due to; pain, nausea, vomiting, diarrhea and findings of ileus attacks are important findings. CT is a valuable tool to help the diagnosis. But in case of any suspicion even if the CT and laboratory is normal, surgeon should never hesitate to perform a laparatomy/laparoscopy to prevent the catastrophic outcomes of a late, delayed intervention.
References
- Koppman JS, Li C, Gandsas A. Small bowel obstruction after laparoscopic Roux-en- Y gastric bypass: a review of 9527 patients. J Am Coll Surg. 2008;206(3):571?84.
- Higa KD , Ho T, Boone KB. Internal hernias after laparoscopic Roux-en-Y gastric bypass: incidence, treatment and prevention. Obes Surg. 2003; 13 : 350-4.
- Wax JR, et al. Intussusception complicating pregnancy following laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2007;17(7):977?9.
- Bebber FE, et al. Pregnancy after bariatric surgery: 39 pregnancies follow-up in a multidisciplinary team. Obes Surg. 2011;21(10):1546?51.
- Ahmed AR, O?Malley W. Internal hernia with Roux loop obstruction during pregnancy after gastric bypass surgery. Obes Surg. 2006;16(9):1246?8.
- Moore KA, Ouyang DW, Whang EE. Maternal and fetal deaths after gastric bypass surgery for morbid obesity. New Eng J Med. 2004;351(7):721?2.
- Leal-González R, et al. Internal hernias in pregnant women with history of gastric bypass surgery: Case series and review of literature. Int J Surg Case Rep. 2013; 4(1): 44?47.
- Torres-Villalobos GM, et al. Small bowel obstruction and internal hernias during pregnancy after gastric bypass surgery. Obes Surg. 2009;19(7):944?50.
- McCollough CH, et al. Radiation exposure and pregnancy: when should we be concerned? Radiographics. 2007;27(4):909?17. discussion 17-8.
|