Abstract
Cystic masses originating from the fetal surface of the placenta have been described by different terms, including chorionic cysts, subchorionic cysts, membranous cysts, and subamniotic hematomas. They occur rarely, and their etiology and clinical importance are still unknown. Herein, we present the case of a placental surface cyst that was diagnosed midtrimester during a routine examination in a patient whose pregnancy was complicated with hypothyroidism.
Keywords :
Placental cyst
, Subchorionic cyst
, Prenatal diagnosis
Turkish Abstract
Plasentanın fetal yüzeyinden kaynaklanan kistik kitleler koryon kistleri, subkoryonik kistler, membranöz kistleri ve subamniotik hematom gibi farklı terimler kullanilarak tarif edilmistir. Nadir görülen bu kistlerin klinik önemi net olarak bilinmemektedir. Biz burada rutin muayene sırasında keşfedilen ve iyi prognoza sahip olan bir plasental yüzey kist olgusunu sunuyoruz.
Turkish Keywords :
, Plasenta kisti
, subkoryonik kist
, prenatal tanı
Introduction
Cystic masses originating from the fetal surface of the placenta have been described by different terms, including chorionic cysts, subchorionic cysts, membranous cysts, and subamniotic hematomas. They occur rarely, and their etiology and clinical importance are still unknown 1,2. Most placental surface cysts that are less than 2 cm in diameter are thought to be harmless 3. Herein, we present the case of a placental surface cyst that was diagnosed in the midtrimester during a routine examination in a patient whose pregnancy was complicated with hypothyroidism.
Case Report
A 29-year-old patient, gravida 2 para 1, had been following up at our hospital due to maternal hypothyroidism, for which she was taking 0.1 mg levothyroxine orally once a day. Her free T4, free T3, and TSH levels were normal from the beginning of the pregnancy.
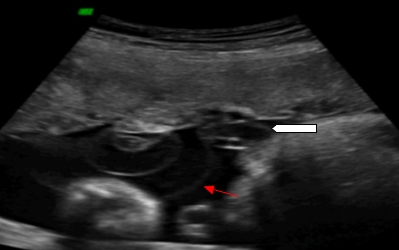
A routine ultrasound examination performed at 28 weeks? gestation revealed a singleton intrauterine pregnancy with a normal and active fetus with measurements compatible with 28 weeks? gestation. However, a complex cystic mass about 3.5 cm in diameter was discovered within the amniotic fluid, close to the insertion point of the umbilical cord into the placenta, generating a ?cyst in the cyst? image (Figure 1). The rest of the placenta was normal in appearance.
The umbilical cord looked normal, and the Doppler measurements of the fetus were also normal. Color Doppler showed no blood flow within the cystic structure. Fetal surveillance was conducted with serial ultrasonography and cardiotocography. The serial ultrasound examinations showed little change in the lesion.
The baby was delivered by Caesarean section following a previous Caesarean section at 39 weeks of gestation, weighing 3000 grams and with APGAR scores of 8 and 10.
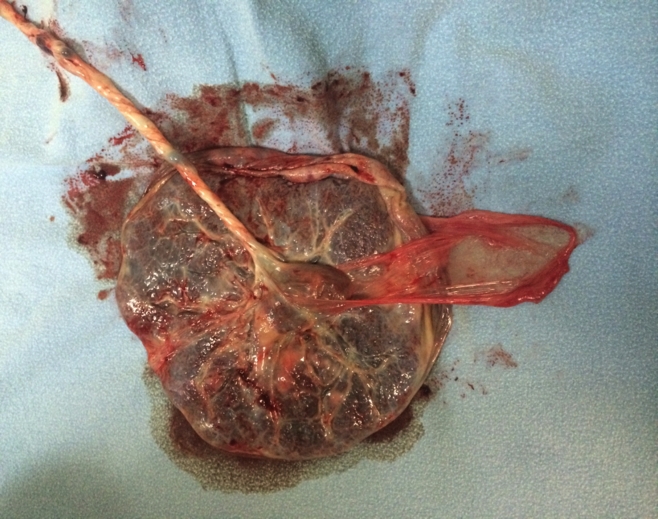
A morphologic evaluation revealed a 550-g, circular placenta measuring 15×13×4 cm. The cord was trivascular, it was inserted 7 cm from the nearest margin of the placenta, and it measured 48 cm in length and up to 1.6 cm in diameter. A fluid-filled cyst was found on the fetal surface of the placenta, located adjacent to but independent from the cord insertion. This cyst measured 4×3.5×2 cm. Interestingly, there was a separate amniotic membrane arising from the cystic area (Figure 2).
A pathological examination of the placenta confirmed a cystic structure arising from the amniotic membrane and extensive subchorionic fibrin deposition.
Discussion
A variety of cysts may be found in the placenta. The differential diagnosis includes subamniotic hematoma, cord cyst, placental lakes, chorioangioma, and vanishing twin 3,4.
Sonographically, placental cysts appear as echo-free cavities under the fetal plate, and they usually remain unchanged on serial scans 3, as in our case. The role of color flow Doppler is important in making the differential diagnosis; it should show no blood flow within the mass 4,5.
On macroscopic examination, these cysts are usually solitary, but there can be multiple cysts as well. They may be central and lie immediately below the chorionic plate. They usually measure less than 2 cm in diameter and tend to occur more frequently in patients with diabetes mellitus or maternofetal rhesus incompatibility. Although small cysts are considered to be obstetrically harmless, cysts larger than 4.5 cm are associated with fetal growth restriction 3.
The relationship between placental cysts and placental vessels is variable. Distended cysts can elevate fetal chorionic vessels, but this condition usually does not interfere with fetal circulation. Although, they usually have no clinical significance, a large subchorionic cyst attached near the umbilical cord insertion may pose a threat to fetal growth 2,3.
In conclusion, particularly large (>4.5 cm) placental surface cysts should be followed closely by ultrasound and color Doppler ultrasonography. Possible fetal growth restriction should be kept in mind.
References
- Brown DL, et al. Placental surface cysts detected on sonography: histologic and clinical correlation. J Ultrasound Med. 2002; 21: 641-6.
- Ferrara N, et al. Subchorionic placental cyst: histopathological and clinical aspects in two cases. Pathologica. 1996; 88: 439?43.
- Raga F, Ballester M, Osborne N, Bonilla-Musoles F. Subchorionic placental cyst: a cause of fetal growth retardation. Ultrasound and color flow Doppler diagnosis and follow-up. J Natl Med Assoc. 1996; 88: 285-8.
- De Leon-Luis J, Oneson RH, Santolaya-Forgas J. Placental surface cyst with contents less echogenic than amniotic fluid on a second-trimester ultrasonographic evaluation. Ultrasound Obstet Gynecol. 2004; 23: 627-8.
- Jauniaux E, Campbell S, Vyas S. The use of color Doppler imaging for prenatal diagnosis of umbilical cord anomalies: report of three cases. Am J Obstet Gynecol. 1989; 161: 1195?7.
Information Presentation
This case report was presented as a poster presentation at the 13th World Congress in Fetal Medicine, June 29?July 3, 2014, Nice, France.
|