Abstract
Sebaceous lymphadenomas are rare benign tumors that are often preoperatively confused with other parotid gland tumors. In this study, a 60-year-old female patient with a 20x15 mm painless mass in the tail of the right parotid gland for two years, is presented. She was diagnosed and treated for sebaceous lymphadenoma in our clinic. The clinical and radiological findings and also histopathological features of this case are discussed with the relevant literature. The treatment of sebaceous lymphadenomas is surgical, and generally partial parotidectomy is sufficient. For a preoperative diagnosis, fine needle aspiration biopsy (FNAB), ultrasonography (USG) and magnetic resonance imaging (MRI) techniques can be used.
Keywords :
Septic Pulmonary Embolism
, Catheter
, Infection
Turkish Abstract
Sebasöz lenfadenomalar, preoperatif tanıda diğer parotis bezi tümörleriyle sıklıkla karışan, oldukça nadir görülen benign tümörlerdir. Bu çalışmada, sağ parotis bezi kuyruğunda lokalize, iki yıldır mevcut, 20x15 mm ebatında, ağrısız kitle şikayetiyle kliniğimizde teşhis ve tedavisi yapılan 60 yaşında kadın hastada saptanan sebasöz lenfedenomun klinik, görüntüleme bulguları ve histopatolojik özellikleri literatür eşliğinde tartışıldı. Sebase lenfadenomaların tedavisi cerrahi olup, parsiyel parotidektomi yeterlidir. Preoperatif tanı için, ince iğne aspirasyon biyopsisi (İİAB), ultrasonografi (USG) ve magnetik rezonans görüntüleme (MRG) teknikleri ayırıcı tanıda kullanılabilir.
Turkish Keywords :
, Septik pulmoner emboli
, Kateter
, Enfeksiyon
Introduction
Septic pulmonary embolism (SPE) is a rare clinical syndrome that manifests itself in cases such as valvular heart diseases, intravenous drug administration and intravenous catheter administration 1. It is characterized by formation of infarct and abscess that emerge when coagulated blood with microorganism meets lungs through the right ventricle of the heart 2. Its morbidity and mortality is high. Early diagnosis, a wide-spectrum antibiotherapy and elimination of the agent are of importance for prognosis 2. The largest series in the literature are mostly related to IV drug users 1. The dialysis catheter-induced septic embolism is a rarely-reported complication 3. This pictorial essay offers interesting radiological findings, clinical characteristics, diagnostic process and treatment of a case with SPE following a dialysis catheter insertion with spectacular radiologic findings of nodular lesions, cavitary lesions and pleural effusion at the same time.
Case Report
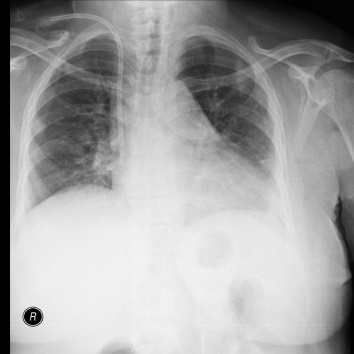
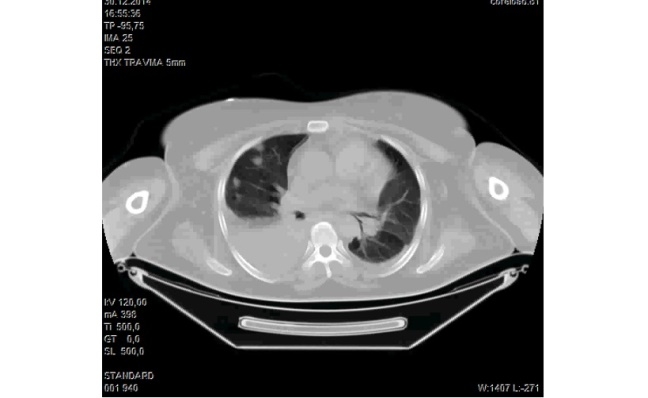
A 55-year old female patient was rushed to the emergency service due to deterioration in general medical condition and fever. Her medical history featured diabetes mellitus, hypertension and chronic renal failure (CRF), and she was undergoing hemodialysis therapy three-days in a week. The patient was operated through A-V fistula, and administered with a temporary hemodialysis catheter through the right internal jugular vein. Having suffered from fever and dyspnea, the patient was referred to the chest diseases clinic for consultation. Fever:39 °C, pulse: 122 bpm., blood pressure 130/80 mmHg, the patient's arterial blood gas analysis revealed pH: 7.34, PCO2:38 mmHg, PO2:57 mmHg, SaO2: 78%. The examination for the respiratory system pointed to bilateral rales. Hemogram result was as follows: White blood cell: 13.1 x10^9/L (4-10x10^9/L), % neutrophil: 87.9% (50-70%), Hemoglobin: 9.7g/dL (11-15 g/dL), C-Reactive protein (CRP): 333 mg/L (0-5 mg/L), Procalcitonin: >100 ng/ml (0-0.046 ng/ml). Serially-administered lung x-rays pointed to newly-emerging bilateral multifocal nodule densities which were tending to cavitate (Figure 1).
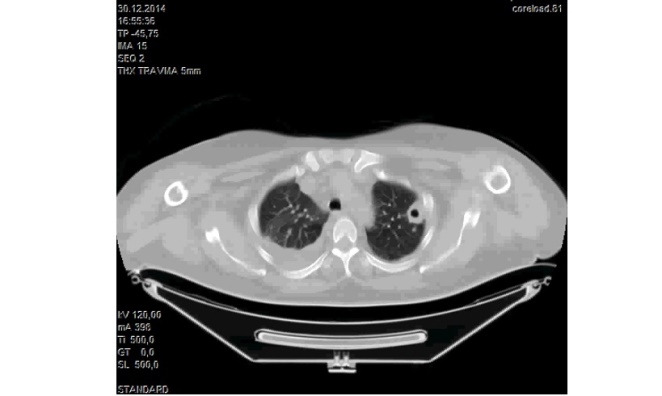
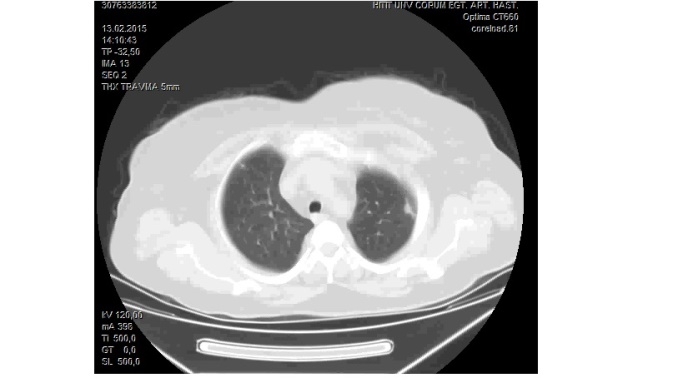
The thoracic CT revealed that both lungs had nodular lesions with the largest one having a13 mmdiameter on the right side and thick-walled cavitary lesions with the largest one having a25 mmdiameter on the left side, and pointed to the bilateral minimal pleural effusion (Figure 2). Echocardiography proved no vegetation and the left ventricular functions were normal while the ejection fraction was 60%.
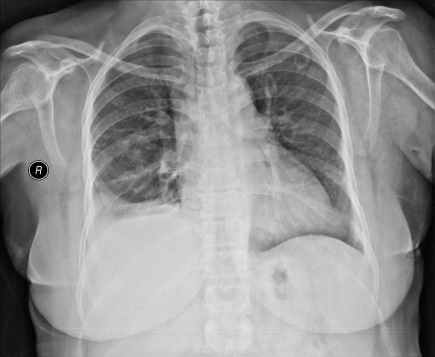
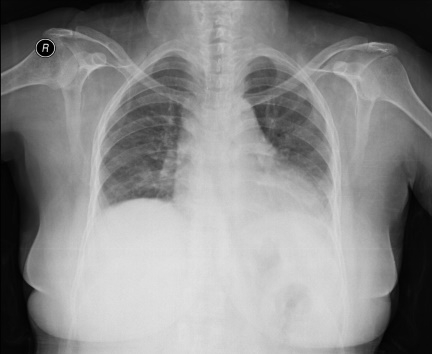
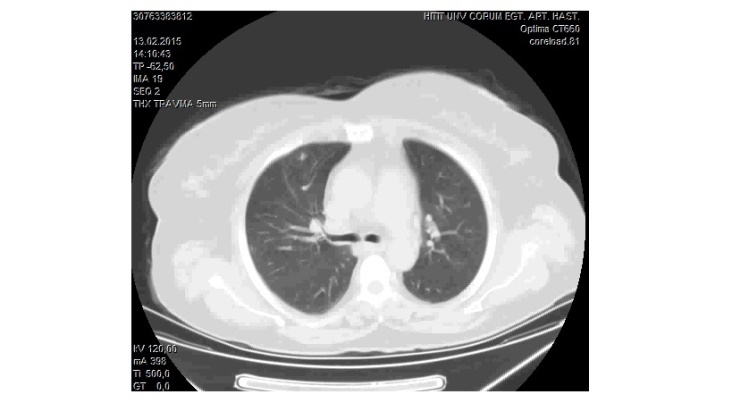
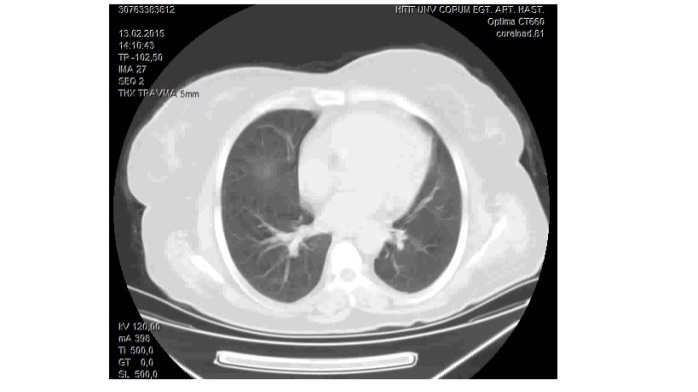
Pleural fluid was found out as exudate as a result of thoracentesis administered in company with right hemithorax ultrasonography. No reproduction was observed in pleural fluid culture. Tuberculosis PCR and BACTEC administered on pleural fluid turned out to be negative. Staphylococcus Aureus reproduced in the blood culture. With a suspicion of catheter-related septic embolism, the catheter was removed, and a therapy of Tigesiclin + Moxifloxacin was initiated in line with the profile of microbiological resistance. During follow-up, the patients fever and acute phase reactants lowered while a clinical improvement was observed; WBC: 7.9x10^9/L (4-10x10^9/L), % neutrophils: 61.5% (50-70%), CRP: 30.1mg/L (0-5 mg/L). After treatment radiologic findings also disappeared (Figure 3).
Informed consent has been taken from the patient during the follow-up period.
Discussion
Septic pulmonary embolism is a rare yet serious disease. While a series with 60 cases was released in 1978, the literature could only offer case presentations in the following years. Among the causes of septic embolism are IV drug usage, infective endocarditis of tricuspid valve, septic thrombophlebitis, suppurative angina, periodontal abscess, purulent infection of soft tissues, intravascular pacemaker and catheters, liver abscess and hemodialysis 1.
Thrombosis formation on the distal tip of central venous catheter is an uncommon complication 4. If the catheter tip contacts the right atrium wall, this probability is higher based on the secondary traumatic endothelium damage. However, central catheters have infection risks just like all foreign bodies. The more prevalent central venous catheters are administered, the more prevalent similar clinical problems manifest themselves 2,5-7. The prevalence of central venous catheter-related bacteremia is 5.3/1000 catheter days 8.
The clinical findings of the septic pulmonary embolism is not specific. The most common findings are fever, dyspnea, chest pain and cough 2.
Septic pulmonary emboli have specific imaging findings. There might be nodules, patchy infiltrates, cavitary lesions and pleural effusion 9. Many cases may feature more than two radiological findings. In addition to patchy infiltrates and pleural effusion, the most common ones are multiple nodules tending to cavitate close to pleura in both lungs 9.
Our case featured peripheral patchy consolidation tending to cavitate bilaterally as well as nodules and unilateral pleural fluid. Fluid was detected in exudate function as a result of the thoracentesis whereas there was no reproduction in the fluid cultures. Following a therapy of antibiotics, a decline was observed in all radiological findings and pleural fluid.
Staphylococcus Aureus is the most common pathogen for IV drug users, soft tissue infection and catheter-related infections. The blood culture results corroborated this situation 2. Our case pointed to S. Aureus reproduction in blood and catheter culture.
For septic pulmonary embolism, it is recommended to immediately take out the infected lesion, catheter or the pacemaker. The empiric treatment of antibiotics should be started without waiting for the blood culture results, and adjusted in line with the culture results 10.
For our case, the empiric treatment of antibiotics was replaced by suitable antibiotics in line with the blood culture results. The dialysis catheter was removed and then reproduction was detected on the catheter tip in line with the blood culture.
Upon a clinical improvement during the follow-up, a decline was observed in lesions as a result of the post-treatment radiological follow-up.
For the treatment of septic pulmonary embolism, the anticoagulant treatment is not usually recommended due to the bleeding risk whereas the anticoagulant treatment is usually preferred in cases of thrombosis or thrombophlebitis 2. For our case, a deep venous thrombosis (DVT) was detected in the right femoral vein as a result of lower limb venous doppler ultrasonography. Therefore, an anticoagulant treatment was administered along with antibiotics in our case. The reason why the diagnosis of septic pulmonary embolism outweighed the pulmonary embolism secondary to DVT in our case, resulted from major fever complaints, peripheral nodular lesions tending to cavitate with a radiological suspicion of septic pulmonary embolism, reproduction in line with blood and catheter culture, and apparent clinical and radiological responses to the treatment of antibiotics.
This essay was presented due to the fact that it was an uncommon hemodialysis catheter-related septic embolism and it had a distinctive radiological appearance. It is important for medical education to show the radiologic findings are how important for accurate diagnosis, and also it is important to eliminate the agent and immediately start with suitable antibiotics along with a detailed clinical history, a physical examination, imaging methods and taking specimens for culture.
References
- MacMillan JC, Milstein SH, Samson PC. Clinical spectrum of septic pulmonary embolism and infarction. Journal of Thoracic and Cardiovascular Surgery. 1978;75(5):670-9.
- Ye R, et al. Clinical characteristics of septic pulmonary embolism in adults: a systematic review. Respirat Med. 2014;108(1):1-8.
- Abid Q, Price D, Stewart MJ, Kendall S. Septic pulmonary emboli caused by a hemodialysis catheter. Asian Cardiovasc Thorac Ann. 2002 Sep;10(3):251-3.
- Yavuzgil O, Ozerkan F, Erturk U, Islekel S, Atay Y, Buket S. A rare cause of right atrial mass: Thrombus formation and infection complicating a ventriculoatrial shunt for hydrocephalus. Surgical Neurology. 1999 Jul;52(1):54-5.
- Baddour LM, Bettmann MA, Bolger AF, et al. Nonvalvular cardiovascular device-related infections. Circulation. 2003 Oct 21;108(16):2015-31. PubMed PMID: 14568887.
- Gilon D, Schechter D, Rein AJ, et al. Right atrial thrombi are related to indwelling central venous catheter position: insights into time course and possible mechanism of formation. Am Heart J. 1998 Mar;135(3):457-62.
- Horner SM, Bell JA, Swanton RH. Infected right atrial thrombus--an important but rare complication of central venous lines. Eur Heart J. 1993 Jan;14(1):138-40.
- National Nosocomial Infections Surveillance (NNIS) System report, data summary from October 1986-April 1998, issued June 1998. American journal of infection control. 1998 Oct;26(5):522-33.
- Richard B. Jaffe EBK. Septic pulmonary emboli. Radiology. 1970;96(3):527-32.
- Liu C, Bayer A, Cosgrove SE, et al. Clinical Practice Guidelines by the Infectious Diseases Society of America for the Treatment of Methicillin-Resistant Staphylococcus aureus Infections in Adults and Children: Executive Summary. Clinical Infectious Diseases. 2011 February 1, 2011;52(3):285-92.
Information Presentation
18th. Annual Congress of Turkish Thoracic Society ?Toraks 2015? Antalya / TURKEY (verbal presentation)
|