Abstract
A 28-year-old female patient presented with complaints of cough that had continued for two months, sputum, and nocturnal sweating. As the sputum acid-fast bacilli was positive, anti-tuberculosis treatment was initiated. In the second month of treatment, pulmonary tuberculosis spread locally to pleura and breast. The case was diagnosed as secondary breast tuberculosis and surgical drainage was added to treatment. In this case report we aim to discuss the secondary form of breast tuberculosis with a discussion of the current literature.
Keywords :
Breast
, Magnetic resonance imaging
, Tuberculosis
, Ultrasonography
Turkish Abstract
Yirmi sekiz yaşındaki bayan hasta iki aydır devam eden öksürük balgam ve gece terlemesi şikayeti ile göğüs hastalıkları polikliniğine başvurdu. Balgamda aside dirençli basil pozitif bulunması üzerine hastaya akciğer tüberkülozu tanısıyla antitüberküloz tedavi başlandı. Tedavinin ikinci ayında akciğer tüberkülozunun plevraya ve memeye lokal yayılımı gözlendi. Olgu sekonder meme tüberkülozu tanısı aldı ve antitüberküloz tedaviye ek olarak cerrahi drenaj yapıldı. Bu olgu sunumuyla, sekonder meme tüberkülozunu, güncel literatür eşliğinde tartışmayı amaçladık.
Turkish Keywords :
, Manyetik rezonans görüntüleme
, Meme
, Tüberküloz
, Ultrasonografi
Introduction
Tuberculosis is one of the earliest diseases known in the world. Breast involvement is a rare form of this disease. While the incidence of breast tuberculosis among all the breast lesions is 0.1% in developed countries, this rate is 4% in developing countries where tuberculosis is endemic1,2. It is differentiated into two categories as primary and secondary. In primary breast tuberculosis, only the breast is affected. In secondary breast tuberculosis, there is a primary tuberculosis focus, apart from the breast. Spreading ways to the breast are; hematogenous, directly by intervention of the thoracic wall or retrograde from the lymph nodes3. The current case report aimed to present secondary breast tuberculosis that is quite rare.
Case Report
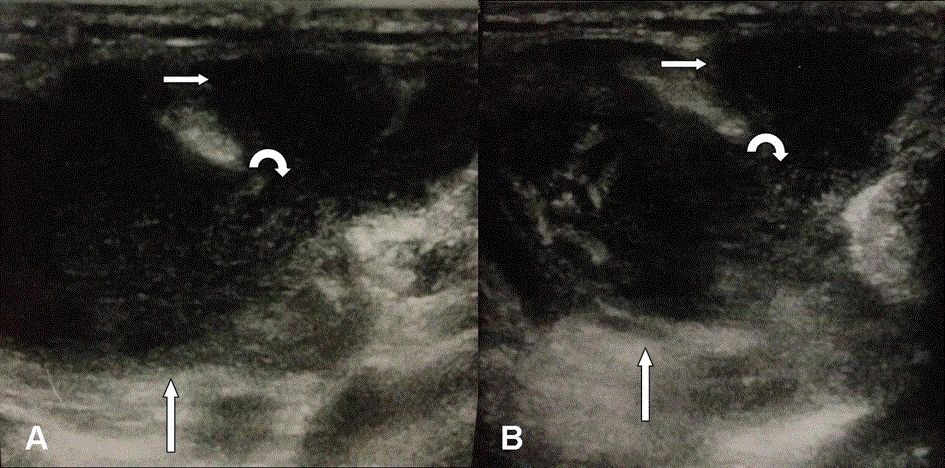
A 28-year-old female patient presented with complaints of cough that had continued for two months of sputum and nocturnal sweating. As the sputum acid-fast bacilli (ARB) was positive, anti-tuberculosis treatment of isoniazid, rifampicin, pyrazinamide, ethambuthol (HRZE) was initiated. In the second month of treatment, pulmonary tuberculosis spread locally to pleura and breast. ARB was positive in the samples taken from pleural fluid and breast abscess. The tuberculin skin test measured 21 mm and sedimentation was 88 mm/hour. Breast US revealed a collection area in the left external quadrant showing association with the pleura (Figure 1 A-B).
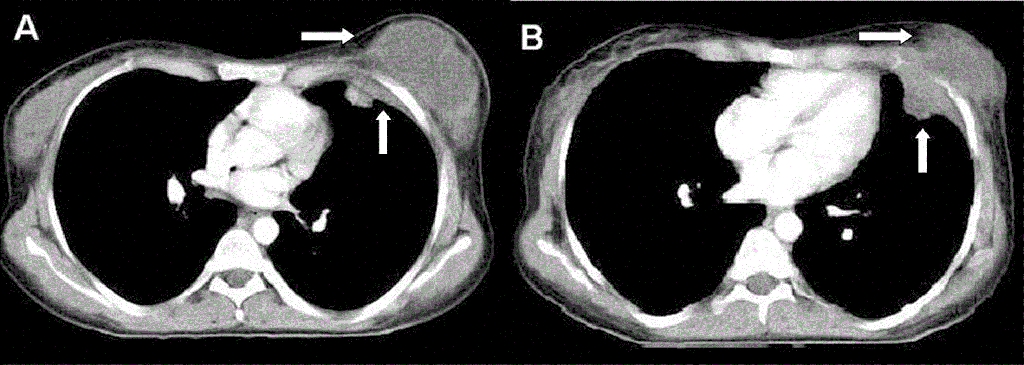
Chest tomography (CT) showed pleural fluid in the left lung upper zone extending to left breast with the parenchymal infiltrations. (Figure 2 A-B).
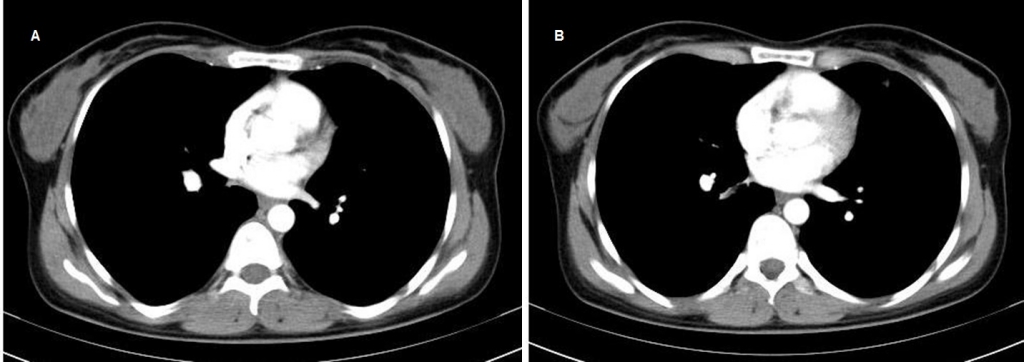
As the symptoms in breast continued, surgical drainage was applied. Antituberculosis therapy consisted of HRZE in thr first three months. Despite of the fact that there was sensitivity to medications, it took 6 months to achieve ARB negative results. Thus HR therapy was completed to one year. After one year of treatment, there was full recovery in the radiologic imaging (Figure 3 A-B).
Discussion
Breast tuberculosis is often seen in the 20-40 years age group of fertile women. The lesion is usually unilateral. Both the left and right breasts are affected at an equally frequent rate. Though the most common involvement is the upper external quadrant, it may be seen anywhere in the whole breast 4. It is argued that pregnancy and the lactation period make the breast susceptible to tuberculosis 5. Our case was in the fertile age group, the lesion was unilateral and in the external quadrant.
The tuberculin skin test is frequently positive. However, positive tuberculin skin test is a non-specific finding. It reflects whether if the individuals? immune system had been contaminated with tuberculosis bacilli previously in an active or passive way. Detection of ARB in the fresh tissue culture is the most important diagnostic criteria, however it is quite difficult even with the procedures of present day. The positive ARB incidence in excisional biopsies of certain breast tuberculosis patients was reported to be between 12% and 22.7% 6,7. Diagnosis is confirmed histopathologically by showing Langerhans giant cells, epithelioid granuloma and lymphohistiocytic aggregates 8,9. In our case, ARB of the material taken from sputum, pleural fluid and breast was positive.
While the incidence of breast tuberculosis in the cases of pulmonary tuberculosis was very low, a 60% incidence of non-breast organ tuberculosis was reported in the cases of breast tuberculosis. These cases are defined as ?secondary breast tuberculosis?. The bacilli might reach to breast tissue hematogenously, directly from adjacent tissues and more frequently by retrograde lymphatic route 4,5. Our case was due to the local invasion of pulmonary and pleural tuberculosis and was evaluated as the secondary form.
Breast infections with fistula formation to skin, tuberculosis should be considered in differential diagnosis. Also the differential diagnosis should include breast cancer, pyogenic breast abscess, actinomycosis infection,(which is quite rare), breast cysts, traumatic fat necrosis, and granulomatous syphilis 5.
In the our case, these were ruled out due to production of direct bacilli.
Without histopathological confirmation, malignancy and breast tuberculosis cannot be differentially diagnosed by imaging procedures alone 10.
Though in the recent past, total excision and even simple mastectomy was performed in the treatment of breast tuberculosis, today it concentrates on anti-tuberculosis treatment as the first choice. It is reported that in a case of lesions with small dimensions anti-tuberculosis treatment alone could be sufficient 5.
If the response to medical treatment is not complete, surgical treatment (cold abscess drainage, extraction of residual mass) is performed. Simple mastectomy must be considered in cases of ulcerative mass with prevalent pain 11. Both abscess drainage and anti-tuberculosis treatment was applied to our case. There was a good response to treatment.
Although nowadays there is a significant decline in tuberculosis incidence due to the application of efficient vaccinations and treatment methods, mycobacterium tuberculosis infections are still a public health problem, especially for developing countries. Secondary tuberculosis of the breast is a rare entity when compared to pulmonary tuberculosis. Tuberculosis should be considered in fistulized breast abscesses, especially in young patients.
References
- Akçakaya A, et al. Tuberculosis of the breast. Breast J. 2005; 11(1): 85-6.
- Tewari M, Shukla HS. Breast tuberculosis: diagnosis, clinical features management. Indian J Med Res. 2005; 122(2): 103-10.
- Haagensen CD. Infections in the breast. Diseases of the Breast. 3th ed. WB Saunders Company: 1986: p. 384-94.
- Harstein M, Leaf HL. Tuberculosis of the breast as a presenting manifestation of AIDS. Clin Infect Dis. 1992; 15: 692-3.
- Khanna R, et al. Mammary tuberculosis: Report on 52 cases. Postgrad Med J. 2002; 78: 422-4.
- Shinde SR, Chandawarkar RY, Deshmukh SP. Tuberculosis of the breast masquerading as carcinoma: a study of 100 patients. World J Surg. 1995; 19(3): 379-81.
- Gupta D, et al. Fine needle aspiration cytology in the diagnosis of tuberculosis mastitis. Acta Cytol. 1999; 43(2): 191-4.
- Sen M, Gorpelioglu C, Bozer M. Isolated primary breast tuberculosis: report of three cases and review of the literature 2009; 64(6): 607-10.
- Akçay MN, et al. Mammary tuberculosis: importance of recognition and differentiation from that of a breast malignancy: report of three cases and review of the literature. World J Surg Oncol. 2007; 5: 67.
- Schwartz GF. Bening neoplasms and ?inflammations? of the breast. Clin Obstet Gynecol. 1982; 25(2): 373-85.
- Jah A, et al. Tuberculosis of the breast: experience of a UK breast clinic serving an ethnically diverse population. Ann R Coll Sung Engl. 2004; 86(6): 416-9.
|