Abstract
Biliary cystadenomas(BCA) are rare hepatobiliary cystic tumors arising from the biliary epithelium. They are more common in middle-aged women and their most being site is the right hepatic lobe. We report the case of a middle-aged woman who underwent cystotomy and drainage for a giant hepatic cystic lesion, of which some characteristics and the clinical presentation were suggestive of hepatic hydatid cyst. Because of the histological analysis of the cyst wall revealed BCA then the patient was taken to operation again and left hepatectomy was performed. BCA and hepatic hydatid cyst have similar radiological characteristics such as multilocular cyst with internal septations. When the multilocular cystic mass was detected in the liver BCA should be kept in the mind.
Keywords :
Biliary cystadenoma
, Hepatic cyst
, Liver resection
, Hepatic hydatid cyst
Turkish Abstract
Biliyer kistadenom (BKA), nadir görülen, biliyer epitelden gelişen hepatobiliyer kistik tümörlerdir. Orta yaş kadınlarda ve karaciğer sağ lobunda daha sık görülürler. Biz karaciğerde dev kistik lezyonu olan ve bazı karasteristik özellikleri ve klinik prezentasyonu kist hidatiği düşündüren, kistotomi ve drenaj ameliyatı uygulanan orta yaşta bir kadın hasta sunduk. Hastanın histopatolojik incelemesi BKA ile uyumlu gelmesi üzerine hasta tekrar ameliyata alınarak sol hepatektomi ameliyatı uygulandı. BKA ve karaciğer kist hidatiği multiloküle kistler ve internal septasyonlar gibi benzer radyolojik özelliklere sahiptir. Eğer karaciğerde multiloküle kistik kitle saptanırsa BKA olabileceği de akılda tutulmalıdır.
Turkish Keywords :
, Biliyer kistadenom
, Karaciğer kisti
, Karaciğer rezeksiyonu
, karaciğer Kist Hidatik
Introduction
Biliary cystadenomas(BCA) are rare hepatobiliary cystic tumors arising from the biliary epithelium. They are characterized by large multiloculated macroscopic lesions and their location is mostly intrahepatic. BCA and hepatic hydatid cyst(HHC) have similar radiological characteristics such as multilocular cyst with internal septations. They are more common in middle-aged women and their most being site is the right hepatic lobe. BCA carries a tendency for local recurrence and a risk of malignant transformation.
We report the case of a middle-aged woman who underwent cystotomy and drainage for a giant hepatic cystic lesion, of which some characteristics and the clinical presentation were suggestive of hepatic hydatid cyst. As, the histological analysis of the cyst wall revealed BCA then the patient was taken to operation again and left hepatectomy was performed.
Case Report
A 49-year-old woman presented in surgical clinic with complaints of coughing and abdominal pain for last three months. She had no other symptoms or medical history of liver disease. On physical examination, she was a well-appearing, non-jaundiced female and no evidence of hepatosplenomegally, lymphadenopathy, or masses; beside this, there was no significant finding including vital sign. Laboratory examination showed normal CA125, CA19.9, a-fetoprotein (AFP), carcinoembryonic antigen (CEA) and liver function tests. A multiloculated ,mixed echo cystic mass of 11.7 cm ×11 cm in the left lobe of liver was detected in abdominal ultrasonography (US). Abdominal tomography(CT) revealed a multiloculated cystic mass of11.5 cm × 11 cm in the left lobe of liver, within daughter vesicles with a possibility of HHC (Figure 1).
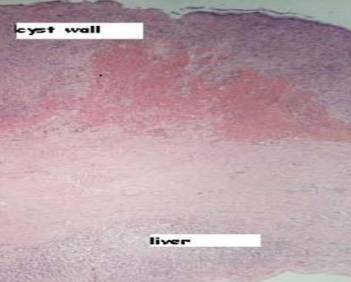
She underwent to exploratory laparotomy. During the operation, a large multiloculated cystic lesion was observed in the left lobe of liver and cystotomy, partial cyst excision and drainage was performed. The histopathological examination of the cyst wall specimen yielded the final diagnosis of the BCA. The transplantation and hepatology council discussed the patient and decided to left lobectomy. Patient underwent to surgery, left lobectomy was performed. The histopathological examination for the resected specimen yielded the final diagnosis of the BCA (Figure 2).
Resection margins of the hepatic parenchyma were free of tumor cell. The patient showed no postoperative complication and was discharged on postoperative seventh day. She is doing well during consecutive follow up of fourteen months.
Discussion
Biliary cystadenoma is a rare cystic neoplasm of unknown aetiology and releated approximately 5% of all the hepatobiliary cystic masses 1. They arise from the intrahepatic or, less frequently, the extrahepatic bile duct. The tumor is thought to form from the obstruction of the congenitally aberrant bile duct or due to the development of ectopic rests of primitive foregut sequestered within the liver . Histologically, cystoadenomas are characterised by the presence of cysts lined with mucinous cuboidal or columnar epithelium 2. BCA is usually atypical symptoms , includes abdominal pain, fullness, nausea and rarely jaundice etc., depending on the location of the tumour 3. Tumor markers are not significant in the diagnosis. For diagnosis US, CT and/or Magnetic resonance imaging (MRI) are the radiological findings and major radiological characteristics of BCA are large multilocular cystic lesions with internal septations and mural nodules. Obstructive jaundice and cholangitis,hemorrhage and cyst rupture are very uncommon, presenting complications of these lesions 4. ERCP may be useful to investigate the communication between the tumor and bile ducts. The differential diagnosis of patients with complex cystic lesions of the liver includes BCA, as well as hydatid cyst, post-traumatic cyst, liver abscess, polycystic disease, hemorrhagic cyst, embryonal sarcoma, primary or metastatic necrotic neoplasm, atypical simple cyst, and biliary intraductal papillary mucinous neoplasm 5,6,7. Imaging studies by US, CT and MRI play animportant role in diagnosis. Characteristic featuresinclude, irregularly thickened wall, sharp demarcation, mural papillae and internal septa, etc. The risk of malignant transformation of BCA to Biliary cystadenoma carcinoma can be as high as 20% 7,8. First option of treatment is the radical excision of the tumor . Operative complete extirpation is essentially important because of considered to be a premalignant lesion. The operation for complete extirpation of lesion may be perform open or laparoscopic surgery according to the surgeon's decision. Mucinous biliary cystadenoma can be radically resected along with the tissue with a 2 cm margin from it.
In our patient symptoms are non- specifik and CT scan revealed a multiloculated cystic mass of the left lobe of liver within like daughter vesicles with a possibility of HHC but the histopathological examination of specimen yielded the diagnosis of the Biliary cystadenoma. BCA and hepatic hydatid cyst(HHC) have similar radiological characteristics such as multilocular cyst with internal septations. When the multilocular cystic mass was detected in the liver , BCA should be kept in the mind .
References
- Dixon E, et al. Cystadenomas of the liver: a spectrum of disease. Can J Surg. 2001; 44: 371 ? 6 .
- Voltaggio L, Szeto OJ, Tabbara SO. Cytologic diagnosis of hepatobiliary cystadenoma with mesenchymal stroma during intraoperative consultation: a case report. Acta Cytol. 2010 ; 54 ( 5 Suppl ): 928 ? 32 .
- Taketomi A, et al. A case of biliary cystadenoma with obstructive jaundice. Oncol Rep. 1998; 5: 833?5.
- Filippi de la Palavesa MM, Vasilescu C, Habersetzer F, Roy C. Biliary cystadenocarcinoma: sonographic and cytologic findings. J Clin Ultrasound. 1999; 27: 210-2.
- Soochan D, Keough V, Wanless I, Molinari M. Intra and extra-hepatic cystadenoma of the biliary duct. Review of literature and radiological and pathological characteristics of a very rare case. BMJ Case Rep. 2012 Apr 4; 2012. doi:10.1136/bcr.01.2012.5497
- Nakagawa M, Matsuda M, Masaji H, Goro W. Successful preoperative diagnosis of biliary cystadenoma with mesenchymal stroma and its characteristic imaging features: report of two cases. Turk J Gastroenterol. 2011; 22: 631-5.
- Soares K, et al.Cystic neoplasms of the liver: Biliary cystadenoma and cystadenocarcinoma. J Am Coll Surg. 2014; 218(1): 119?28.
- Vyas S, et al. Hepato-biliary cystadenoma with intraductal extension: unusual cause of obstructive jaundice. J Gastrointest Cancer. 2011 May 28 [Epub ahead of print].
Information Presentation
Presented as a poster at the 24th Conference of the Asian Pasific Association for the Study of the Liver (APASL 2015), 12-15 March, 2015, Istanbul, Turkey
|