Abstract
Congenital heart disease has been reported as frequent as %4 of infants and Tetralogy of Fallot (ToF) is seen nearly 1/4000 live births. Some of them can reach older age and can remain fairly asymptomatic much of their live. A case had been reported as 83 years old ToF with no correction. We corrected a 60 years old ToF who stands oldest patient we had been operated by ToF. This case has focused attention on successful follow up of a case with repaired ToF in the middle?aged.
Keywords :
Tetralogy of Fallot
, Cyanotic congenital heart disease
, Pulmonary atresia
Turkish Abstract
Fallot tetralojisi (ToF), 1/4000 doğumda ve %4 infant doğumda görülen konjenital kalp hastalığıdır. Bu hastaların az bir kısmı ileri yaşlara kadar yaşayabilir ve tüm yaşamları boyunca asemptomatik olabilirler. Herhangi bir müdahale yapılmayan 83 yaşında bir vaka daha önce bildirilmiştir. Biz burada, 60 yaşındaki ToF?li erkek hastamızın başarılı takibini ve cerrahi onarımını sunduk. Bu hastamız kliniğimizde ameliyat ettiğimiz en yaşlı ToF vakası idi.
Turkish Keywords :
, Fallot tetralojisi
, Siyanotik konjenital kalp hastalığı
, Pulmoner atrezi
Introduction
TOF is one of the most common forms of congenital heart disease. Tetralogy of Fallot (ToF) occurs in nearly 1/4000 live births and 4% of infants born with congenital heart disease. The initial diagnosis can make by echocardiography. Some of them can reach older age and can remain fairly asymptomatic much of their live. In addition, ToF corrective surgery in a older age is associated with peri-operative problems. Perioperative assessment, successful surgical strategies and attentive intensive care monitoring are very important in order to reduce morbidity and mortality. A case had been reported as 83 years old ToF with no correction. We corrected a 60 years old ToF who stands oldest patient we had been operated by ToF.
Case Report
A sixty years old male presented with dyspnea on mild exertion and mild cyanosis. The medical history had include no palliation or other typical symptoms. In addition, he had a 1/6 mid-systolic murmur on the aortic fields. Moderate hypoxemia and minimaly hypocapnia was detected in his blood gas analysis. Routine blood count and also biochemical measurements were normal. In chest X-ray, lungs were normal, cardiothoracic rate was increased with widened aortic knob.
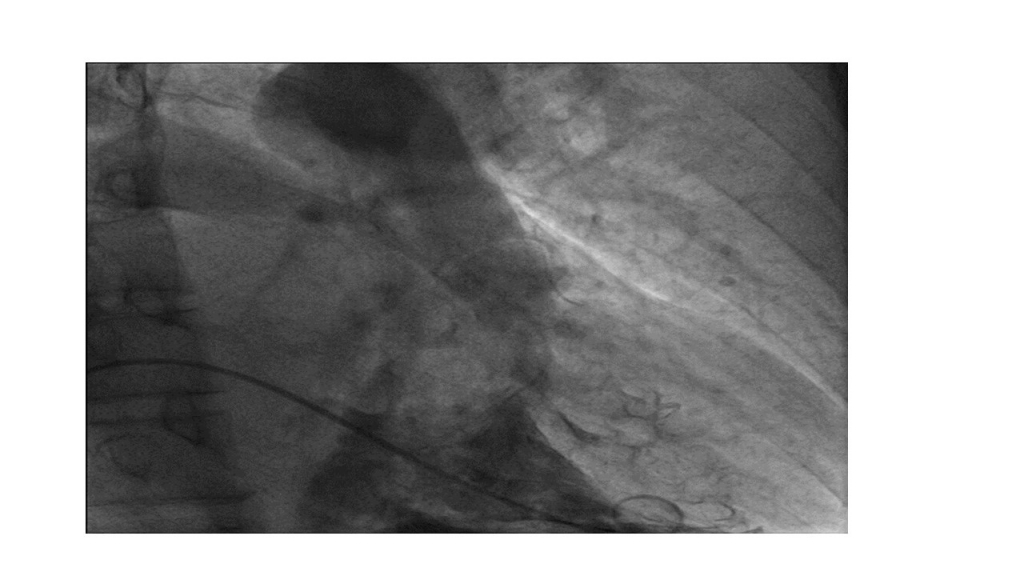
Patient inspected by echocardiography, angiography afterwards in epicentral but had no ToF diagnosis. Therefore we studied for complete diagnosis at our clinic repeating Echo and angiography. Echocardiographically, dextropositioned aorta, overriding, subaortic large ventricular septal defect (VSD), severe pulmonary stenosis was presented. The angiography examination revealed with subvalvuler level 40 mmHg and pulmonary valvular level 80 mmHg moderate right ventricular outflow tract obstruction (RVOTO)(Figure 1).
The diagnosis was based on the presence of a large perimembranous VSD with over 50% aortic overriding. Infundibular obstruction reported. The McGoon index was reported as 2. Evidence confirmed ToF diagnosis with severe pulmonary stenosis in 6th decade of life.
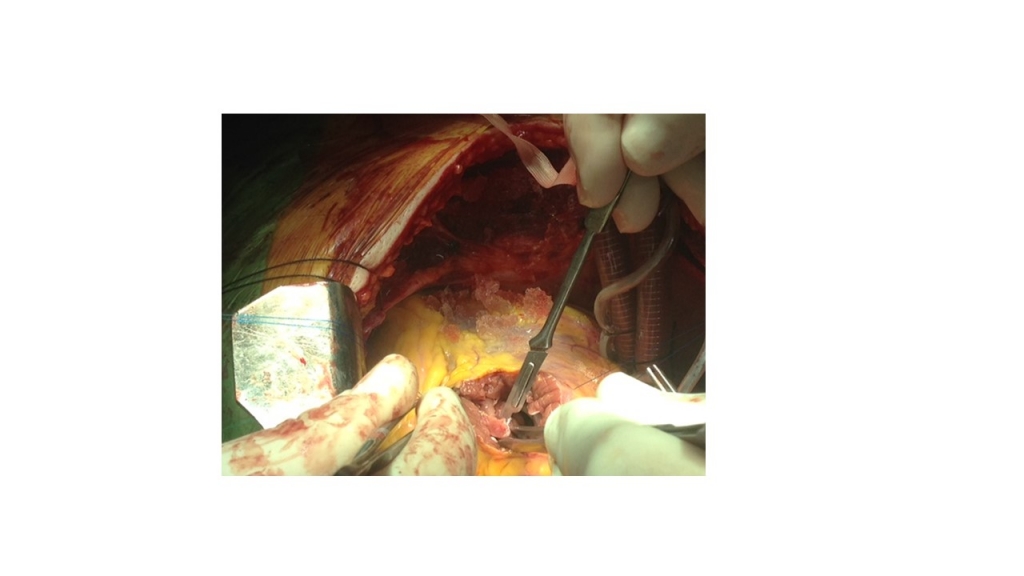
Profound hypothermia (280C) was used. Repair made by transannular patch augmentation. The muscular ventriculo?infundibular fold excised (Figure 2).
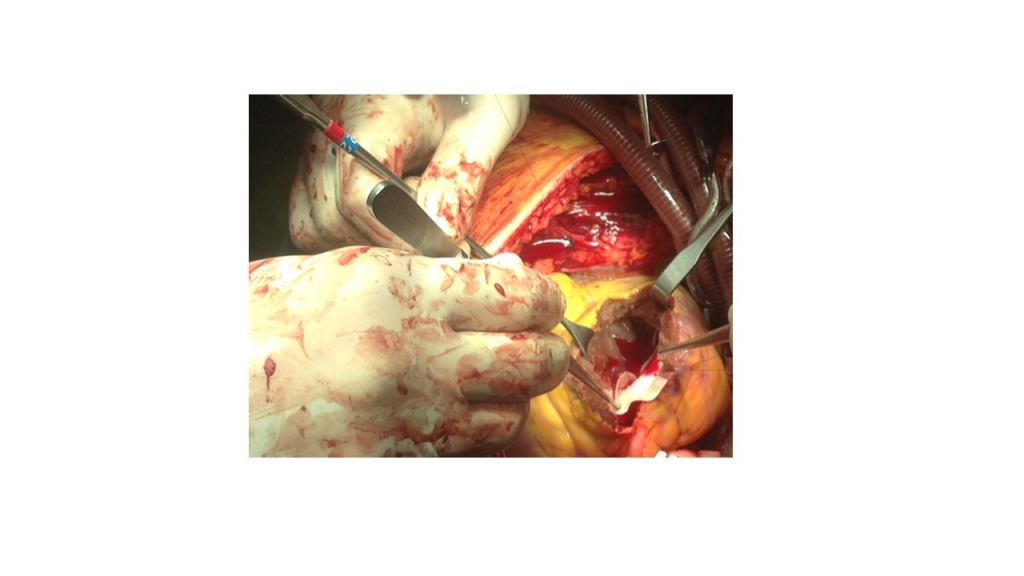
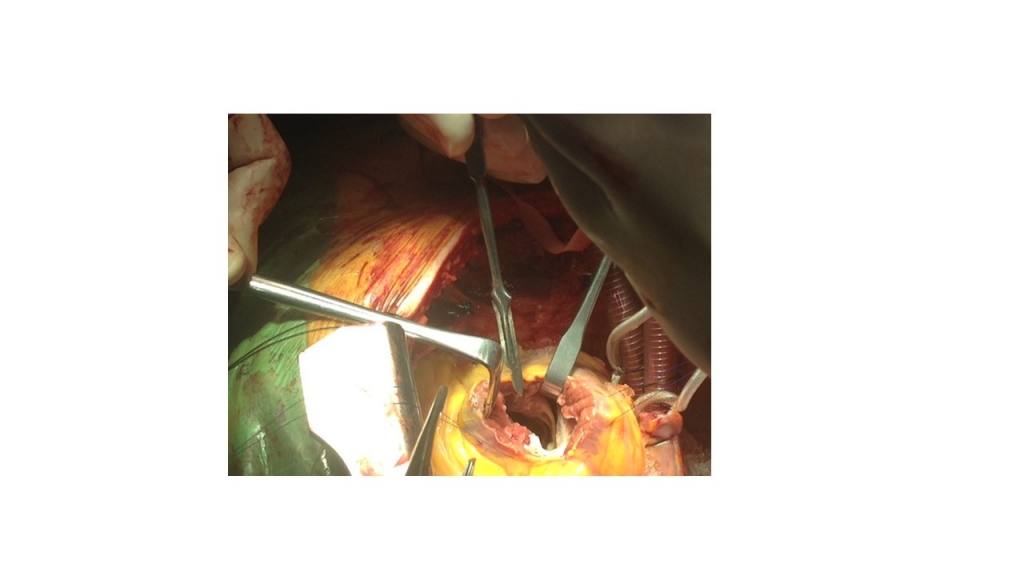
Large perimembranous VSD repaired with patch. Transannular bovine patch to relieve RVOTO was used to preserve pulmonary valve function. The pulmonary vascular resistance was low. The gradient was 10 mmHg (Figure 3-4). Ultra?filtration was used.
In the follow-up period, patient discharged without complication. There had been reported rare cases undiagnosed reach elderly. We think it was an interesting case of successful repaired ToF management with middle-aged (60).
Discussion
Tetralogy of Fallot is a very common cyanotic congenital heart disease, which presents with typical symptoms in infancy or childhood 1. Fetal karyotyping include analysis of microdeletion of chromosome 22q11.2 2-4. First surgical repairs were introduced in the 1950s. Rate of survival at 40 years without any symptom is only 3% 1-2. Echocardiographically, the diagnosis of ToF can now be made antenatally 3-5. Prostaglandin infusion can protect and avoid from potential hypoxic cerebral damage with maintain ductal patency 6. Although open repair still remains the standart approach. On the basis of mortality and physiological outcomes, the optimal age for the elective repair reported 3 to 11 months of age 3. Surgical repair must be performed by experienced teams. These patients also had significant comorbidites which made them eligible for open repair. If clinically indicated, initial palliation can benefit in the symptomatic infants to one of elective primary repair around the age of 6?months or earlier. Studies reported no benefit in delaying elective repair of ToF after the end of the first year 1-3. Undergo primary rather than staged repair are recommended for symptomatic infants over six months 7. Also, primary repair recommend to down to the age at which the individual hospital risk of a shunt 1-4.
Longer term study reported on primary repair in excellent surgical results of 61 consecutive neonates with 95% five year actuarial survival 4. Pulmonary artery (PA) size is considered a major risk factor as to whether primary repair of ToF. This remains the case for older children or adults. In addition, the size of the main PA and its ratio to the ascending aorta in the older-aged cases with ToF reflects the severity of outflow tract obstruction.
We report a patient with tetralogy of fallot diagnosed at 6th decade. ToF can reach elderly can remain asymptomatic for some time. ToF in elderly can successfully corrected. If pulmonary valve can not be preserved pulmonary valve replacement (PVR) should be always kept in mind. We preserved pulmonary valve in our case and patient improved eventfully with a short hospitalization.
References
- E. Shinebourne, S. B. Narayan, J. S Carvalho. Tetralogy of Fallot: from fetus to adult. Heart 2006;92(9):1353-9.
- Gibbs J L, et al. Survival after surgery or therapeutic catheterisation for congenital heart disease in children in the United Kingdom: analysis of the Central Cardiac Audit Database for 2000?1. BMJ. 2004;328:611?5.
- Van Arsdell GS, et al. What is the optimal age for repair of tetralogy of Fallot? Circulation. 2000 Nov 7;102(19 Suppl 3):III123-9.
- Hirsch J C, Mosca R S, Bove E L. Complete repair of tetralogy of Fallot in the neonate: results in the modern era. Ann Surg. 2000;232:508?14.
- Babu?Narayan S V, et al. Ventricular fibrosis suggested by cardiovascular magnetic resonance in adults with repaired tetralogy of Fallot and its relationship to adverse markers of clinical outcome. Circulation. 2006; 113:405?13.
- Peres LC, Bekhit M, Johki R. A tetralogy of fallot associated with a stenotic pulmonary valve and agenesis of the ductus arteriosus in a 13-week-old fetus: the role of postmortem examination. Pediatr Dev Pathol. 2012; May-Jun:15(3):240-4.
- Hussain FT, Grogan M, Dearani JA. Surgical repair of tetralogy of fallot at age 83. World J Pediatr Congenit Heart Surg. 2012; Oct 1:3(4):518-20.
|