Abstract
Inferior turbinates are important anatomical structures in the formation of nasal airflow resistance. That's why, minimal alterations in the size of inferior turbinates can alter nasal airflow and cause nasal blockage. Some anatomical variations of turbinates are available in the literature and frequency of anatomical variations increased with widespread use of paranasal CT. Case reports of the middle turbinate variations are common and most of them are bullous chonca but pneumatization of inferior turbinate is rare. In this case report, we present a 24-year-old female patient who had nasal obstruction and atypical facial pain due to left side inferior turbinate pneumatization which form a common cavity with maxillary sinus.
Keywords :
Inferior turbinate
, Maxillary sinus
, Pneumatization
, Common cavity
Turkish Abstract
Alt konkalar, nazal hava akımı direncinin oluşumunda önemli anatomik yapılardır. Bu nedenle, alt konka boyutundaki küçük değişiklikler hava akımını belirgin derecede etkileyerek burun tıkanıklığına neden olur. Nazal konka anatomik varyasyonları, literatürde mevcuttur ve bilgisayarlı tomografi kullanımının yaygınlaşması ile birlikte varyasyonların saptanma sıklığı artmıştır. Orta konka anatomik varyasyonları ile ilgili olgu sunumları yaygındır ve çoğunluğu konka bülloza şeklindedir fakat alt konka pnömatizasyonu nadirdir. Bu yazımızda, pnömatize alt konka ve maksiller sinüsün birlikte havalanma gösterdiği ortak kavite varyasyonu nedeniyle oluşan burun tıkanıklığı ve atipik baş ağrısı şikayeti ile başvuran 24 yaşında bayan hasta sunulmuştur.
Turkish Keywords :
, İnferior konka
, Maksiller sinüs
, Pnömotizasyon
, Ortak kavite
Introduction
Turbinates are important anatomic structures of the lateral nasal wall.1,2 Most of the air inhaled pass through between the lower and middle turbinate. Inferior concha is placed at internal nasal valve region and responsible for heating, filtration and directing of nasal airflow and 2/3 of nasal air flow resistance.2,3,4 Therefore, even small changes in the size of the inferior turbinate significantly affect nasal airflow.3,4 The widespread use of computed tomography in the diagnosis has increased the incidence of anatomic variations of nasal turbinates.5,6
Due to the impact on the sinus drainage, anatomic variations of the middle turbinate have been studied frequently in the literature. Most commonly, concha bullosa is described.1 Anatomical variations of the inferior turbinate are important in clinical practice. It can cause nasal obstruction, and atypical facial pain.4,7 Altough it is not a life threatening condition, nasal obstruction can interfere with the quality of life. Chronic nasal obstruction is a common disorder and if septal defects are excluded, the main structure contributing to this problem is the inferior turbinate.2,7 Anatomical variations of inferior turbinates such as inferior turbinate pneumatization , bifid inferior turbinate, inferior turbinate hypoplasia described before are available in the literature.1-11 Pneumatization of the inferior turbinate are rarely seen as an anatomic variation.1-4,8,10,12,13 Although embryologic origins of the inferior tubinate and maxillary sinus are different, in our case, there was an inferior turbinate pneumatization which formed a common cavity with the maxillary sinus. We discussed this rarely seen case report under the light of literature.
Case Report
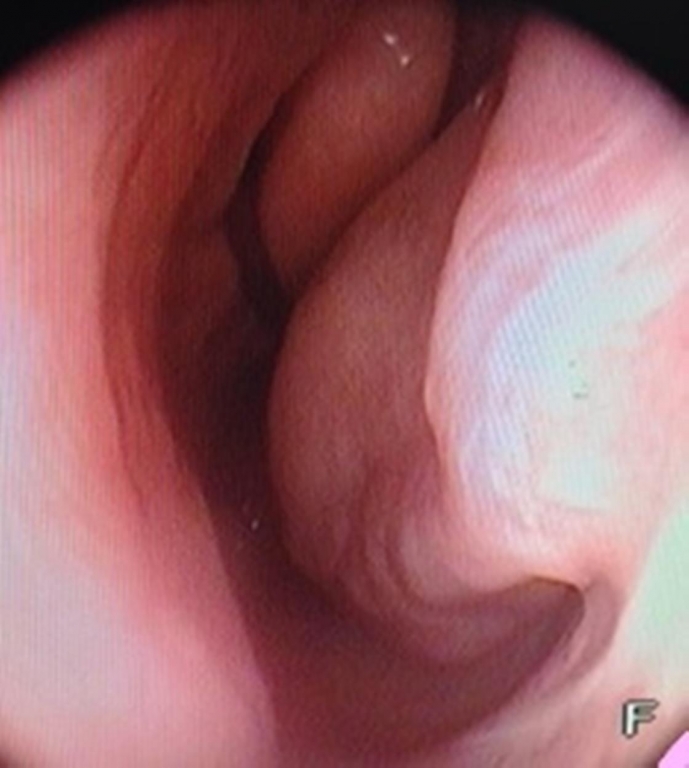
24-year-old female patient presented with complaints of nasal congestion and occasional headache was admitted our clinic. On physical examination, the patient's septum deviation to the right side and the right inferior turbinate hypertrophy was detected. The endoscopic view of left nasal cavity is shown in Figure 1.
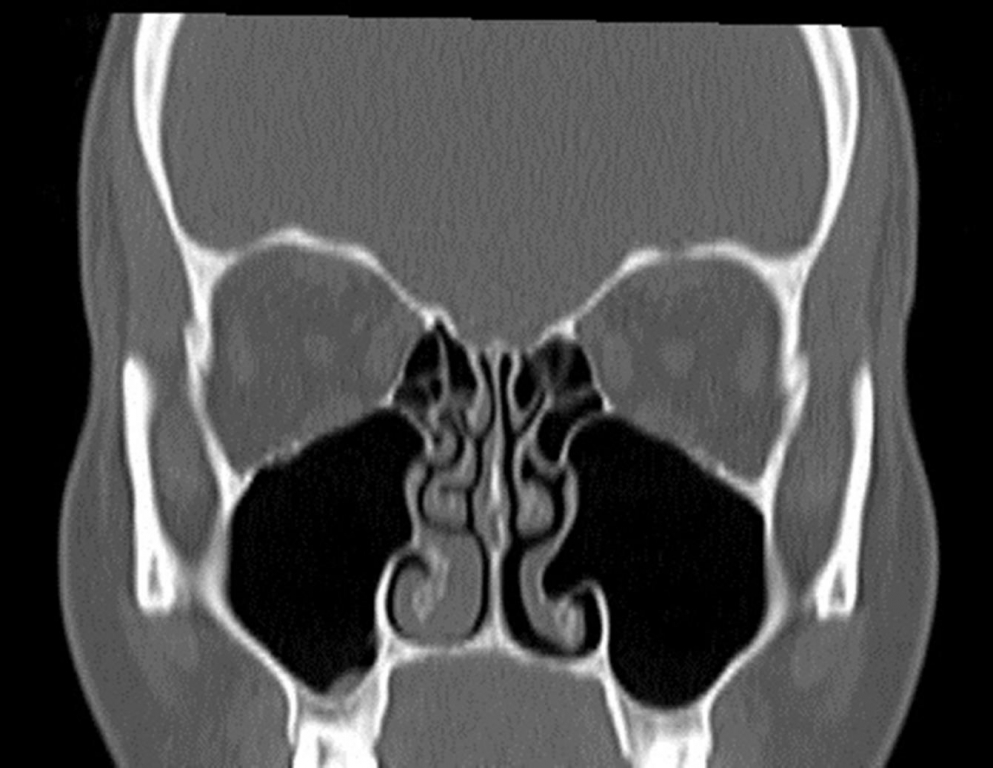
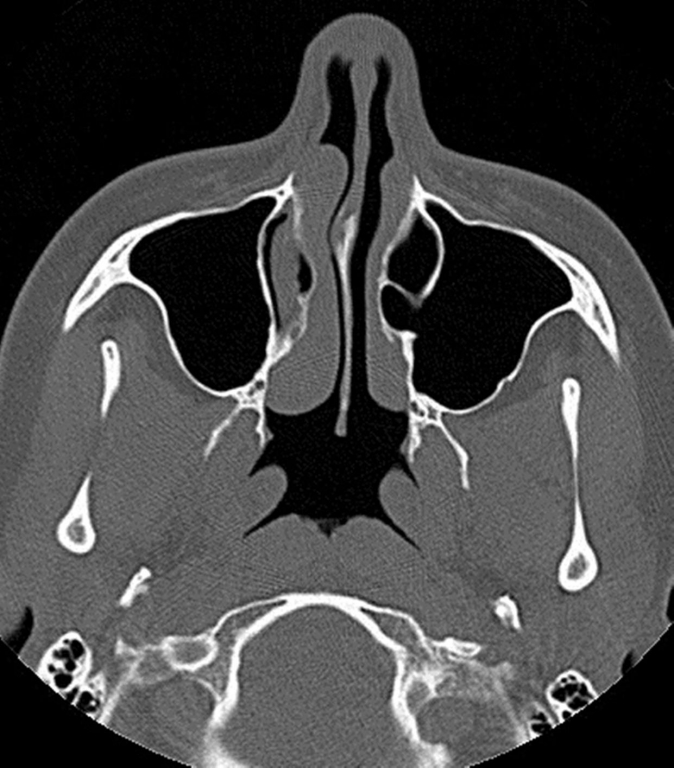
Paranasal sinus CT scan showed the right inferior turbinate hypertrophy and right septum deviation. However, the left pneumatized inferior turbinate showed continuity into the maxillary sinus space and made a common pneumotized cavity (Figure 2-3).
Surgical intervention was not considered for the patient. Medical treatment and clinical follow-up was recommended. Despite of their different embryological origin, inferior turbinate and maxillary sinus formed a common pneumatized cavity.
Discussion
Turbinates are anatomical structures of nasal cavity consisting of bones and surrounding soft tissue. Superior and middle turbinate are parts of the ethmoid bone whereas inferior turbinate is a separate bony structure. The precursors of the turbinates occurs in the 7th week of fetal life. The origin of the inferior turbinate is maxilloturbinal projection while the middle and lower turbinate and also maxillary sinuses are etmoturbinal. Turbinates are easily identifiable by 16 weeks. Inferior turbinate is developed by enchondral ossification and during this period, any alteration on process may lead to kinds of variations. The frequency of anatomic variations of the turbinates has been increased with the widespread use of CT.3,6,7,11
Inferior turbinates are important anatomic structures in the formation of the internal nasal valve and forming nasal airflow resistance. Therefore, anatomic variations of the inferior turbinate which causes nasal congestion are the most common cases at practice. Small changes in the size of the inferior turbinate greatly affects nasal airflow.1-8 These inferior turbinate variations were defined as ; pneumatization of the inferior turbinate, inferior turbinate agenesis, accessory inferior turbinate, inferior turbinate hypoplasia, bifid inferior turbinate and paradoxical inferior turbinate.1-11 Regarding the prevalence of anatomic variations of the inferior turbinate, a study reported the prevalence as 2 %.7
Turbinates may be pneumatized, but this is the most common in the middle turbinate and the least in the inferior turbinate.8 There are two hypothesis about this variation. Inferior turbinate has two chondral lamella and two seperate ossification centers. This centers fuse during development. During this period the epithelium may be invaginate into the double lamella and cause pneumatization. Another hypothesis suggest that; during fetal life, maxillary sinus pneumatization extends into the inferior turbinate.3,13 Our case is compatible with this hypothesis. Also, a case of pneumatization of inferior turbinate which form common cavity together with maxillary sinus as in our case was found in the literature.3,5,12,13 Yang et al. reported this pathology in 8 out of 18 inferior turbinate pneumatization cases.13 To the best of our knowlodge it is believed that our case is the ninth of this variation. The pathology in our patient was detected during control CT evaluation, but it may be symptomatic clinically.
By endoscopic examination, it can not be possible to distinguish the inferior turbinate pneumatization and turbinate hypertrophy. Therefore paranal sinus computed tomography in the assessment of anatomic variations of this region is extremely important.4 In our case, there were no findings on physical examination but on CT scan; inferior turbinate pneumatization demonstrated that there was continuity with the maxillary sinus and they together created a common cavity despite the development from different embryological structures.
In the presence of an anatomic variation such as common cavity of maxillary sinus and inferior turbinate as in our case, by the surgical approach to inferior turbinate like lateralization or submucosal resection, maxillary sinuse can be damaged because of absence of an anatomical barrier to protect the maxillary sinus from contaminated inspiratory airflow. Therefore, appropriate approach for this pathology was thought to be medical treatment in our case.
Anatomic variations of the inferior turbinate are frequently seen in patients.7 Clinical symptoms like atypical facial pain and nasal congestion can be observed in the pathology of the inferior turbinate. Determination of anatomic variations by using CT scan, making an accurate diagnosis and choosing the appropriate treatment modality is very important.
References
- Ozcan KM, et al. Anatomical variations of nasal turbinates. J Craniofac Surg. 2008;19:1678-82.
- Çankaya H, et al. Pneumatization of the concha inferior as a cause of nasal obstruction . Rhinology 2001; 39:109-11.
- Pittore B, Al Safi W, Jarvis SJ. Concha bullosa of the inferior turbinate: an unusual cause of nasal obstruction. Acta Otorhinolaryngol Ital. 2011; 31:47-9.
- Uzun L, Uğur M, Savranlar A. Pneumatization of the inferior turbinate. European Journal of Radiology Extra 2004; 51:99-101
- Passàli D, et al. Treatment of hypertrophy of the inferior turbinate: long-term results in 382 patients randomly assigned to therapy. Ann Otol Rhinol Laryngol. 1999; 108:569-75.
- Lee Lee SY, et al. Bilateral accessory inferior turbinates and secondary middle turbinates. Jpn J Radiol. 2012; 30:530-32.
- Yasan H, et al. Alt konka anatomik varyasyonlarının sıklığı. KBB-Forum 2006; 5: 12-4
- Dawlaty EE. Inferior concha bullosa--a radiological and clinical rarity. Rhinology. 1999; 37:133-5.
- Lee JH, Koh SH. A variant form of bifid inferior turbinate. Ear Nose Throat J.2011; 90:E33-4.
- Ozcan C, Gorur K, Duce MN. Imaging study of the month massive bilateral inferior concha bullosa. Ann Otol Rhinol Laryngol 2002; 111:100-1
- Naiboğlu B, Yaylacı A, Oysu C. Paradoxical giant inferior concha. Ear Nose Throat J. 2011; 90:E18-9.
- Unlu HH, et al. Inferior concha bullosa. J Otolaryngol. 2002; 31:62-4.
- Yang BT, et al. CT appearance of pneumatized inferior turbinate. Clin Radiol. 2008; 63:901-5.
Information Presentation
10. Türk Rinoloji Kongresi, 22-25 Mayıs 2014, Belek, Antalya
|