Abstract
The most common primary tumor of the heart is myxoma and it is mostly detected in left atrium. Symptoms due to atrial myxoma frequently appear as a result of intracardiac obstruction over mitral valve caused by the tumor. Neurologic findings are rarely seen in atrial myxoma patients, however, these neurologic symptoms can be fatal. Atrial myxoma usually originates from foramen ovale region of the interatrial septum. Less frequently, it can atypically originate from right atrium, right ventricle, left atrial appendage, anterior and posterior wall of left atrium, left ventricle or valvular surface.
Keywords :
Myxoma
, Left atrium
, Stroke
Turkish Abstract
Miksoma, kalbin en sık görülen primer tümörüdür ve çoğunlukla sol atrium yerleşimlidir. Atriyal miksomaya bağlı semptomlar, sıklıkla tümörün yol açtığı mitral kapak üzerinde intrakardiyak tıkanma sonucu görülür. Miksomalı hastalarda nörolojik bulgular nadiren görülür, ancak bu nörolojik belirtiler ölümcül olabilir. Miksoma genellikle septumun foramen ovale bölgesinden kaynaklanır. Daha az sıklıkla, atipik olarak sağ atriyum, sağ ventrikül, sol atriyal apendiks, anterior ve sol atrium, sol ventrikül veya kapak yüzeyinin arka duvarından kaynaklanabilir. Bu yazımızda, miksomalı kırk beş yaşındaki kadın hasta sunulmuştur.
Turkish Keywords :
, Miksoma
, Sol atrium
, Strok
Introduction
The most common primary tumor of the heart is myxoma and it is mostly detected in left atrium. Symptoms due to atrial myxoma frequently appear as a result of intracardiac obstruction over mitral valve caused by the tumor. Neurologic findings are rarely seen in atrial myxoma patients, however, these neurologic symptoms can be fatal 1. Atrial myxoma usually originates from foramen ovale region of the interatrial septum. Less frequently, it can atypically originate from right atrium, right ventricle, left atrial appendage, anterior and posterior wall of left atrium, left ventricle or valvular surface 2.
Case Report
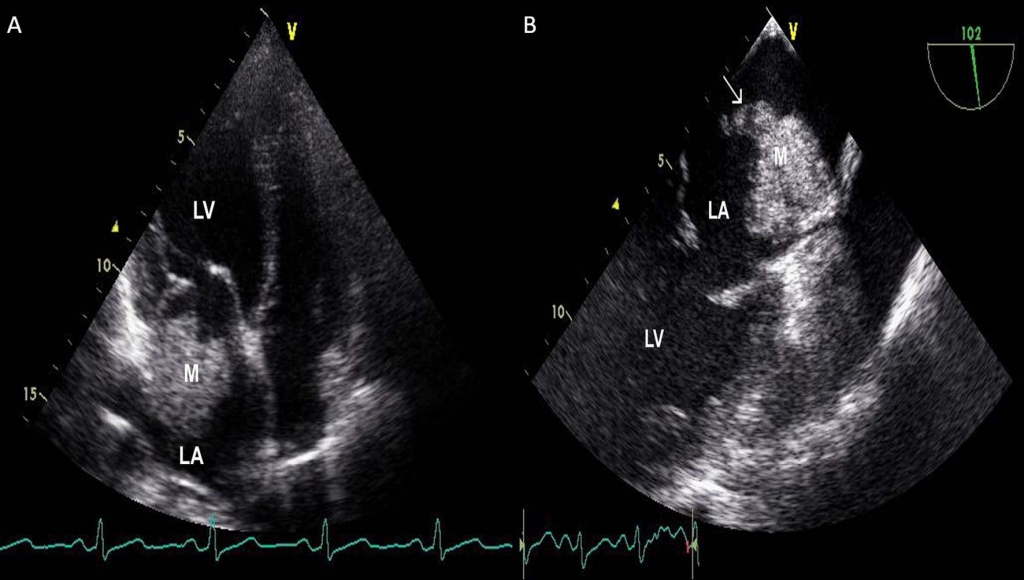
A 45 years old female patient was admitted to our emergency clinic by her relatives with the findings of left hemiparesis, left hemiplegia and aphasia. Her physical examination revealed somnolance with limited cooperation and orientation. Arterial blood pressure was 135/75 mmHg with a pulse of 95 bpm. Babinski sign was detected in left lower extremity with hemiparesis and 4/5 hemiplegia in left lower and upper extremities and central facial paralysis on the left side of the face. Cardiovascular system examination showed mild tachycardia with normal S1 and S2, and a 2/6 grade systolic murmur at mesocardiac area. Electrocardiography revealed sinus tachycardia. In cranial CT, an image consistent with ischemic stroke was detected in right parietal lobe. In transthorasic echocardiography (TTE) about 3x4 cm sized mass was found adjacent to the left atrial lateral wall (Figure 1A). The patient was fallowed under standart neurologic therapy with anticoagulation (enoxaparine sodium 0,6 ml 2x1 subcutaneously). After clinical stabilization and relief of neurologic findings, a transesophageal echocardiography (TEE) was performed for better evaluation of localization, size and nature of the mass. A 34x33 mm mass arising from left atrial appendage with fibrillary thrombi adherent to it was detected in TEE (Figure 1B).
After complete clinical recovery, the patient was operated at first month of her admission. During operation, the atrial myxoma was accessed after thoracotomy and left atriotomy and great amounts of free thrombi in left atrium were aspirated. A 5x3 cm sized gelatinous mass originating from left atrial appendage with a smooth contour was observed adjecent to the anteroposterior commissure of the mitral valve. After suturing its stalk, the mass was excised successfully. The defect on left atrium was closed by a pericardial patch and left atrium was then closed by continuous sutures. The excised mass was consistent with myxoma macroscopically. In histopathological examination of the mass, uniform shaped eosinophilic spindle cells with starry extensions were observed on a myxoid ground among muscle fibrils, thrombi and calcification areas. These findings were compatible with a cardiac myxoma including dystrophic calcification. In postoperative TEE, the mass was shown to disappear completely (Figure 2A and 2B).
Discussion
Although myxoma is a very rarely seen condition as a primary tumor of the heart, it is the most common type among primary cardiac tumors 3. Myxoma originates mostly from left atrium 4. It originates frequently from foramen ovale region of interatrial septum. However, it was reported that it was located atypically in right atrium (15-20%), in left atrial appendage, on anterior and posterior wall of left atrium, in left or right ventricle or on valvular structures 5. Our case with its left atrial appendeal origin, is a rarely seen myxoma case according to the region of origination.
Symptoms due to cardiac myxoma are defined by a classical triad. This triad includes: intracardiac obstruction, systemic embolic events, and constitutional symptoms 6. The most common cause of symptoms among clinical spectrum is intracardiac obstruction. In previous studies, the incidence of any symptom as a first clinical sign of myxoma due to cerebral emboli was reported to be 8% 7. Systemic emboli in a case with myxoma occurs due to embolization of pieces separated from tumor or adherent thrombi to distal vascular areas 8. In our case, it is apparent that fibrillary thrombi on the mass and/or pieces of myxoma itself resulted in cerebrovascular emboli.
Common tendency for time to surgery in myxoma cases is operation early after diagnosis. Surgical treatment is recommended as soon as possible because of the risk of valvular obstruction and systemic embolization 9.
Herein, we demonstrated a case of cardiac myxoma originated from left atrial appendage and caused cerebrovascular emboli with a stroke as its first presentation. Cardiac myxoma clinically can be presented by stroke. Left atrial myxoma should be considered in differential diagnosis of cerebrovascular emboli especially in young subjects and surgical excision must be performed as soon as possible after clinical stabilization.
References
- Pinede L, Duhaut P, Loire R. Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases. Medicine 2001;80:159-72.
- Van Trigt P, Sabiston DC. Tumors of the heart. In: Sabiston DC, Spencer FC, editors. Surgery of the chest. 5th ed. Philadelphia: Saunders; 1990. p. 1901?19.
- Oto Ö. Okutan H. Kutluk K. Stroke ve Miksoma. GKDC Dergisi 1998; 6: 493-497
- McAllister HA, Fenoglio JJ. Tumors of the Cardiovascular System. Washington, DC: Armed Forces Institute of Pathology, 1978.
- Van Trigt P, Sabiston DC. Tumors of the heart. In: Sabiston DC, Spencer FC, editors. Surgery of the chest. 5th ed. Philadelphia: Saunders; 1990. p. 1901?19.
- Peters MN, Hall RJ, Cooley DA. The clinical syndrome of atrial myxoma. JAMA 1974;230:695?701.
- Aggarwal SK, Barik R, Sarma TC, Clinical presentation and investigation findings in cardiac myxomas: new insights from the developing world Am Heart J 2007;154:1102-7.
- Tipton BK, Robertson JT, Robertson JH. Embolism to the central nervous system from cardiac myxoma. Report of two cases. J Neurosurg 1977;47:937?940.
- Kaplan M, et al. Kardiyak miksoma: 45 olguluk deneyim. Türk Göğüs Kalp Damar Cer Derg. 2002;10:11?4.
|