Abstract
Cystic lymphangioma is a rare benign congenital tumour characterised by an abnormal accumulation of lymphatic fluid. Primary lymphangioma is more frequent in males and 80% of cases are in patients under the age of five. It is most commonly located in the mesenteric area of the small intestine. It is thought to occur as a result of the proliferation and dilatation of the lymphatic sacs due to developmental defects of lymphatic vessels. As it is usually seen after surgical procedures and chemotherapy due to lymphoma, it may also occur primarily (1, 2). Rokitansky first made the definition of a cystic mass containing lymph fluid in 1842 (3), and it was defined by Mori in 1955 after the hysterectomy for cervical cancer (4). Ultrasonography and computed tomography have 85% sensitivity for the diagnosis. The recommended method of treatment is total excision due to low recurrence rate (12-17%). Aspiration of the cyst is not an effective method and almost always results in recurrence Is being investigated because of abdominal pain, sagittal, and therefore we have diagnosed the patient discussed lymphangioma
Keywords :
Lymphangioma
, Paraaortic
, Surgery
Turkish Abstract
Özet Kistik lenfanjiyom lenf sıvısının anormal bir birikimi ile karakterize nadir görülen benign konjenital bir tümördür. Primer lenfanjiom, erkeklerde daha sıktır ve % 80, beş yaşın altındaki hastalarda görülmektedir. Yaygın olarak, en çok ince bağırsağın mezenterik bölgesinde yer almaktadır. Lenf damarlarının gelişimsel kusurları nedeniyle lenfatik keselerinin çoğalması ve dilatasyonu sonucu olarak ortaya çıktığı düşünülmektedir. Genellikle, cerrahi operasyon sonrası ve lenfoma nedeniyle kemoterapi sonrası görüldüğü gibi, primer olarak da oluşabilir. İlk kez 1842?de, Rokitansky tarafından lenf sıvısı içeren bir kistik kitle tanımı yapılmış ve 1955 yılında da Mori tarafından, serviks kanseri için histerektomi operasyonu sonrası lenfanjioma tanımlanmıştır. Ultrasonografi ve bilgisayarlı tomografi tanısı için% 85 duyarlılığa sahiptir. Tedavi için önerilen yöntem, düşük nüks oranı (% 12-17) nedeniyle lenfanjiomun total olarak çıkarılmasıdır. Karın ağrısı nedeniyle araştırılırken, lenfanjiom tanısı konan ve opere ettiğimiz hastayı tartıştık.
Turkish Keywords :
, Lenfanjiom
, Paraaortik
, Cerrahi
Introduction
Cystic lymphangioma is a rare benign congenital tumour characterised by an abnormal accumulation of lymphatic fluid. Primary lymphangioma is more frequent in males and 90% of cases are in patients under the age of five. It is most commonly located in the mesenteric area of the small intestine. It is thought to occur as a result of the proliferation and dilatation of the lymphatic sacs due to developmental defects of lymphatic vessels. As it is usually seen after surgical procedures and chemotherapy due to lymphoma, it may also occur primarily 1,2. Rokitansky first made the definition of a cystic mass containing lymph fluid in 1842 3, and it was defined by Mori in 1955 after the hysterectomy for cervical cancer 4. Ultrasonography and computed tomography have 85% sensitivity for the diagnosis. The recommended method of treatment is total excision due to low recurrence rate (12-17%). Aspiration of the cyst is not an effective method and almost always results in recurrence 3,5. Is being investigated because of abdominal pain, sagittal, and therefore we have diagnosed the patient discussed lymphangioma.
Case Report
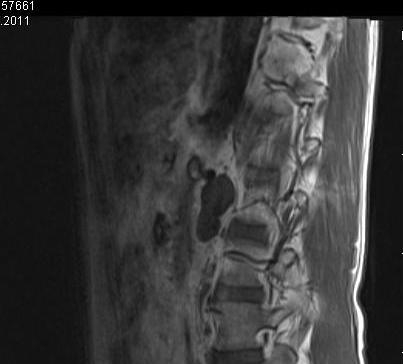
A 55 year-old male patient was complaining of occasional back pain. The physical and laboratory evaluation was normal. After considering the paravertebral cystic lesion as lymphangioma on MRI( magnetic resonans imaging), imaging, the patient was admitted for surgery. In the MR imaging revealed a lesion, lymphangioma, which was 47×20mm? in size, had multi-loculated, lobulated contours, that was located in the anterior paravertebral distance along L2 to L3 vertebral corpus, and was hypo-intense on T1-AG and hyper-intense on T2-AG, showing continuity through left retro-aortic area to inter-aortocaval area, and showing no contrast enhancement. (Figure1, 2)
The patient was diagnosed with para-aortic lymphangioma and underwent elective surgery under general anaesthesia. (Figure 3)
The mass, which was thought to be lymphangioma approximately at the level of L1, was explored and removed after sparing the sympathetic ganglia towards posterior to the aorta. The patient, who had no post-operative complications, had taken food orally on the second post-operative day and was discharged with instructions for the seventh day. Histopathological examination of the excised cystic tissue revealed a tissue sample suggesting CD: 31 and CD: 34 positive lymphangioma. (Figure 4)
Discussion
Lymphangioma is the cystic masses containing lymph fluid resulting from trauma or other injuries; it can also be seen after lymphatic duct pathologies, surgical procedures in which extensive lymphatic dissection is performed, renal transplantation, radical hysterectomy, chemotherapy for lymphoma, and vascular surgical procedures 6,7. Primary lymphangioma is benign neoplasm of lymphatic ducts. While it is seen in 0.5% of children within the first decade of life, its incidence is 0.1% in young adults and those of older ages. While approximately 80% of primary lymphangiomas are seen in children less than five years of age and 95% are seen in the neck and axillary region, 5% are seen in mesentery, the abdominal organs, lungs and mediastinum 8,9.
Retroperitoneal localisation has been reported in 1% of cases 9. Primary intra-peritoneal and retroperitoneal cystic lymphangiomas are rare tumours which are generally found as a small number of case reports in international literature can invade adjacent tissue and organs 5,9. Although retroperitoneal primary lymphangiomas are benign tumours and usually have an asymptomatic course, they can cause non-specific symptoms such as abdominal pain, nausea, vomiting and distension as a result of haemorrhages due to the erosion and torsion of cysts, or as a result of compression and invasion to the adjacent organs such as the ureter and intestines 3,6. Lymphangiomas are thin-walled cystic lesions that consist of microscopic or macroscopic cysts associated with each other. Cysts have a chylous, serous or haemorrhagic character, as well as may contain a mixture of these. As the lesions are asymptomatic because of their small dimensions, they are detected incidentally in the radiological examinations for other reasons as in our case 3. Lymph-angiography shows the relationship of the lymphatic system. However, it is an invasive method and has no benefit in lymphangiomas that are not associated with the lymphatic system. Ultrasonography, computed tomography and MRI are diagnostic methods 6. The signal intensity of most lymphangiomas are equal to or lower than the surrounding muscles in the T1-weighted series on MRI, which is called hypo-intensity, and is higher in T2 weighted series depending on the liquid content of the cystic mass, which is called as hyper-intensity 9,10. In our case, we observed a lesion without contrast enhancement, which was hypo-intense in the T1-weighted series and hyper-intense in the T2-weighted series. The differential diagnosis of lymphangiomas includes multi-loculated acid, enteric, mesenteric and Echinococcosis cysts, it can be difficult to be distinguished due to the similar imaging findings. CT can be used in this case. Hydatid cyst should be considered in the differential diagnosis as it is commonly seen in our country. Definitive diagnosis is made by histopathological evaluation as cystic lymphangiomas have no pathognomonic radiological findings. Several different treatment methods were applied. These include surgical excision, aspiration, percutaneous radiotherapy, laparoscopic drainage and sclerotherapy 3,5,7,11. Spontaneous regression has also been reported as a treatment method especially in children 3,8. Aspiration is not a definitive treatment, but can be applied when urgent decompression is needed 5. However, several different publications have reported that percutaneous aspiration and sclero-therapy have a recurrence rate of 100%, and incomplete excision has a recurrence rate of 40 to 50% 1,3,6,7. The appropriate method of treatment is complete resection 2. Segmental intestinal resection may be needed if cysts are adhered to the wall 1,2. Inadequate surgical resection almost always ends with recurrence 4,9. In studies conducted, it has been reported that recurrence rates were ranged from 12 to 17% in patients who underwent macroscopic total excision and recurrence rates were significantly lower than the other therapeutic procedures. Lack of recurrence during a three-year follow-up and with USG examination is sufficient criterion for definite improvement 1,3.
In the literature, the recurrence rate after incomplete excision and aspiration has clearly been reported to be close to 100% in the treatment of patients with lymphangioma. Aspiration and sclero-therapy does not give satisfactory results, due to the fact that lymphangioma is multi-loculated in many cases. The macroscopic complete excision should be performed for the exact treatment of the lesion, as presented in our case.
References
- Steyaert H, et al. Abdominal cystic lymphangioma in children: benign lesions that can have a proliferative course. J Ped Surg. 1996; 31:677-80.
- Chau G, King K, Su C, Lui W. Retroperitoneal cystic lymphangioma in adults. Int Surg. 1993; 78:243-6.
- Lorken M, Marnitz U, Manegold E,et al. Intraabdominal lymphangioma. Chirurg. 2001; 72:72-7.
- Mori N. Clinical and experimental studies on the so called lymphocyst which develops after radical hysterectomy in cancer of the uterin cervix. J. Jap Obstet Gynecol Soc. 1955; 2:178-203.
- Golematis B, Georgakakism A, Klonis G. Lymphatic cysts of the retroperitoneal space. Could epiploplasty be the method of choice? Am J Gastroenterol. 1997; 67:84-5.
- Takiff H, et al. Mesenteric cysts and intra-abdominal cystic lymphangiomas. Arch Surg. 1985; 120:1266-9.
- Poulos JE, Presti ME, Philips N, et. al. Presentation and management of lymphatic cyst of the colon: report of a case. Dis Colon Rectum. 1997; 40:366-9.
- Huis M, Balija M, Lez C, Szerda F, et al. Mesenteric cysts. Acta Med Croatia. 2002; 56:119-24.
- Levy A, Cantisani V. Abdominal lymphangiomas: Imaging features with pathologic correlation. AJR. 2004; 182:1485-91.
- Jain S, et al. Mesenteric lymphangioma ? diagnosis by multi-slice spiral CT. IJRI. 2002; 4.580-2.
- Türk E, Duman H, Baş Y. Cystic abdominal lymphangioma in children: report of two cases. J Exp Clin Med. 2011; 28: 79-82.
|