Abstract
It is very difficult to establish a diagnosis of tuberculoma when intracranial space-occupying mass lesions are detected without any symptoms of tuberculous infection. Besides, tuberculoma is generally seen as a single focus. In a scarce number of case reports potential multifocality of tuberculomas have been indicated. Images obtained by computed cranial tomographic (CCT), and magnetic resonance (MRI) imaging techniques are not specific for tuberculomas. Need for surgical interventions has decreased after development of antituberculostatic drugs. Therefore, tuberculomas should be considered in the differential diagnosis of other intracranial space-occupying lesions.
Herein, we wanted to demonstrate a case without any typical symptoms of tuberculosis presenting with multifocal intracranial tuberculomas which can be confused with intracranial space-occupying mass lesions especially metastatic lesions.
Keywords :
Intracranial mass
, tuberculoma
, metastasis
Turkish Abstract
Tüberküloz enfeksiyonu belirtileri olmaksızın kafa içi yer kaplayan oluşum saptandığında tüberkülom tanısı koymak çok zordur. Ayrıca tüberkülom genellikle tek odak şeklinde görülür. Az sayıda olgu bildiriminde çok odaklı olabildiği bildirilmiştir. Kafa içi tüberkülomların bilgisayarlı beyin tomografisi (BBT) ve manyetik rezonans görüntüleme (MRG) yöntemleri ile görünümleri spesifik değildir. Antitüberküloz ilaçların gelişiminden sonra cerrahiye duyulan ihtiyaç azalmıştır. Bu sebeple tüberkülomların diğer kafa içi yer kaplayan lezyonların ayırıcı tanısında mutlaka göz önünde tutulması gerekir.
Bu olgu sunumunda kafa içi yer kaplayan lezyonlarla özellikle metastatik lezyonlar ile karıştırılabilen, tüberküloza ait belirgin bir semptomu olmayan, çok odaklı kafa içi tüberkülomları olan bir olguyu sunmak istedik.
Turkish Keywords :
, Kafa içi kitle
, tüberküloma
, metastaz
Introduction
Brain metastases seen in nearly 40 % of cancer patients with systemic disease are important causes of morbidity, and mortality in these patients.1 Primary malignacies which most frequently metastasize to brain are lung cancer, breast cancer, colorectal cancers, renal cell carcinoma, and malignant melanoma.2 Breast, colon, and renal cell carcinomas frequently cause unifocal brain metastases, however generally multiple metastases develop in melanoma, and lung cancer 1. Primary disease is not found in 15 % of the patients with brain metastasis.1
Radiological images of brain metastases are not specific. Generally they demonstrate ringform staining. In cases with ringform stained lesions should suggest other lesions with similar staining characteristics in the differential diagnosis. Among them brain abscesses, toxoplasmosis, granulomas (tuberculosis, sarcoidosis) demyelinizing lesions, primary brain tumours, primary central nervous system lymphomas, stroke, bleedings, and traumas can be enumerated.3
Herein, we presented an asymptomatic tuberculosis patient with intracranial tuberculoma manifesting itself only as a space-occupying lesion which must be absolutely considered among intracranial space-occupying lesions.
Case Report
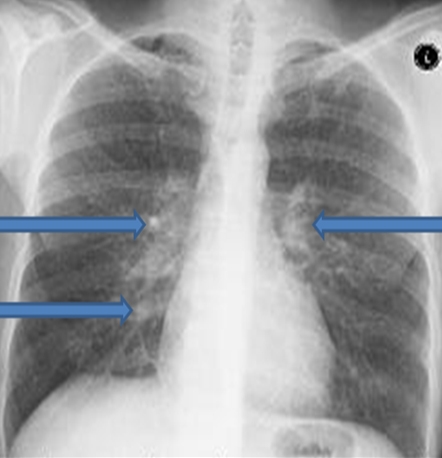
A 31-year old male patient presented to our outpatient clinics of our department of internal medicine. His physical examination revealed physiological respiratory sounds with a body temperature of 36.7 ?C. His neurological examination was unremarkable. His laboratory test parametres were as follows; WBC, 8.190/mm3; hemoglobin 12.1 g/dl; platelets, 399.000/mm3; erythrocyte sedimentation rate (ESR) 57 mm/h; and C-reactive protein (CRP) 31.09 mg/dl. Blood biochemical, coagulation tests, and hepatitis markers were within normal limits. Multiple calcified areas, and reticular changes were observed on chest radiograms (Figure 1).
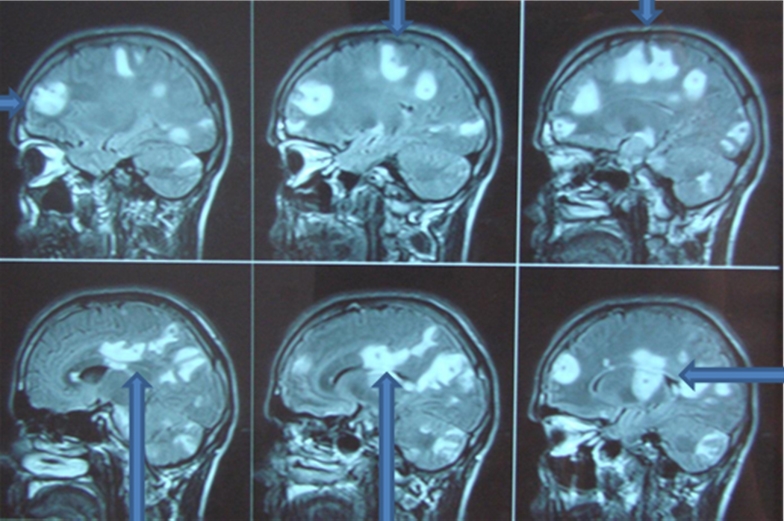
On cerebral MRI, contrast-enhanced ringform lesions were observed in cerebral, and cerebellar hemispheres bilaterally, and brain stem, and asymmetrical enlargements were seen in occipital horns bilaterally, and left ventricular corpus (Figures 2).
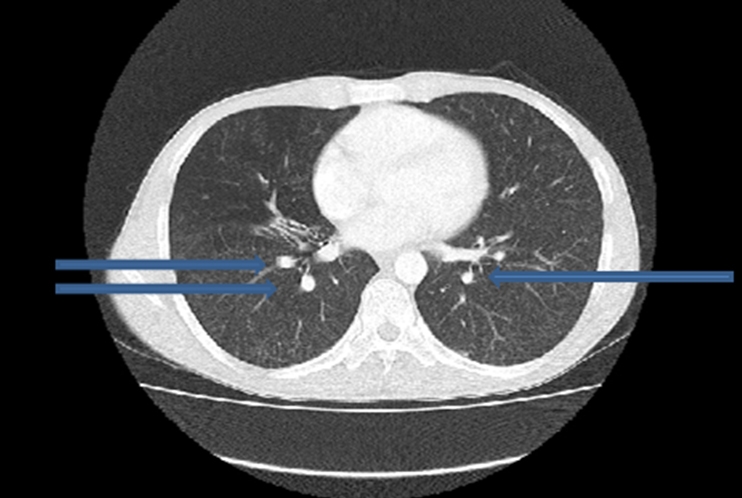
During systemic cancer screening tests performed to rule out the presence of a potential metastatic mass, on thoracic CT images suggesting calcified, and noncalcified millimetric lymph nodes in the mediastinum, diffuse millimetric nodular lesions, and sequelar changes in pulmonary parenchyma were observed (Figure 3). On abdominopelvic CT, liver, gallbladder, pancreas, both kidneys, and other abdominal, and pelvic structures were evaluated as within physiologic limits.
As an outcome of all these findings, the patient was referred to the department of chest surgery for bronchoscopic examination. Samples from bronchoalveolar lavage fluid obtained under the guidance of bronchoscopy revealed the presence of alveolar macrophages, neutrophilic leukocytes, and lymphocytes. On slides prepared, any evidence of malignancy, and specific infection was not seen. In the same biopsy material any abnormal finding was not detected apart from minimal chronic inflammation.
In examinations performed with the possible suspicion of metastatic intracranial mass, any focus of malignancy was not found. However because of the detection of high fever, and increased C-reactive protein, and erythrocyte sedimentation rate necessitated consultation with the department of infectious diseases. The patient had undergone diagnostic spinal tap (LP). Results of biochemical tests performed on cerebrospinal fluid (CSF) samples were as follows; differential blood cell counts were in favour of lymphocytic dominancy; glucose, 21.9 mg/dl; chloride (Cl), 108.1 mEq/L; total protein, 7202 mg/; and lactate dehydrogenase (LDH), 903 U/L. Concurrent serum biochemical test values were as follows; glucose, 127 mg/dl; Cl, 91.1; total protein 7.07mg/L; and LDH 260 U/L. All of these test results were considered in consistent with central nervous system tuberculosis. Besides, acid-fast bacilli (AFB) staining positivity of CSF samples were detected in two successive tests. Then antituberculosis treatment was initiated. Afterwards, the patient with a poor health state experienced respiratory, and then cardiac arrest before his death on the 7 th day of his therapy.
Discussion
In nearly one fifth of the patients with extrapulmonary metastases, tuberculosis manifests itself as meningoencephalitis, while in only 1 % of the patients intracranial tuberculoma develops.4 Intracranial tuberculomas are more frequently encountered in developing countries. They are is more often observed in immunocompromised patients, especially in HIV positive cases.5
It is challenging to diagnose a case with tuberculoma in aysmptomatic tuberculosis patients with established intracranial space-ocupying mass lesion Tuberculomas are usually seen as unifocal lesions. Only 15-34 % of the cases can have multifocal tuberculomas.6 CCT, and MRI images are not specific for tuberculomas.3,7 Conventional MRI, and diffusion-weighted MRI techniques can aid in diagnosis.7 As in our case, tuberculomas can present themselves with symptoms of intracranial space-occupying mass lesions. Tuberculomas can be observed in various regions such as cerebral parenchymal, epidural, sellar or even spinal intramedullary locations.8-10, 11 In the differential diagnosis, primary or secondary cerebral tumours, toxoplasmosis, bacterial or fungal abscesses, and neurocysticercosis should be considered.12,13
In our patient, systemic symptoms such as high fever, nocturnal sweating, and weight loss were not detected. MRI images demonstrating contrast-enhanced multiple ringform masses with surrounding severely edematous zone, and lack of any tuberculous symptoms, and signs suggested the presence of metastatic masses as first possibilities. However, we couldn?t find any focus of malignancy during our investigations.
In conclusion, similar to our case, in the differential diagnosis of especially asymptomatic cases of tuberculous infection with intracranial space-occupying lesions, probable existence of tuberculoma(s) should be kept in mind, and investigations targeted to that end should be conducted.
References
- Nguyen TD, Abrey LE: Brain metastases: old problem, new strategies. Hematol Oncol Clin North Am 2007; 2: 369-388.
- Peak S, Abrey LE: Chemotherapy and the treatment of brain metastases. Hematol Oncol Clin North Am 2006; 20:1287- 1295.
- Draouat S, Abdenabi B, Ghanem M, Bourjat P: Computed tomography of cerebral tuberculoma. J Comput Assist Tomogr 1987; 11: 594-597.
- Basta M, Lydakis C, Daskalogiannaki M, Schiza S, Siafakas NM: Multi-focal tuberculosis with multiple intracranial tuberculomas in a non-immunocompromised patient. Respir Med. 2001; 95: 841-843.
- Martínez-Vázquez C, Bordón J, Rodríguez-González A, de la Fuente-Aguado J, Sopeña B, Gallego-Rivera A, Martínez-Cueto P: Cerebral tuberculoma: a comparative study in patients with and without HIV infection. Infection 1995; 23: 149-153.
- Bouchama A, al-Kawi MZ, Kanaan I, Coates R, Jallu A, Rahm B, Siqueira EB: Brain biopsy in tuberculoma: the risks and benefits. Neurosurg 1991; 28: 405-409.
- Basoglu OK, Savas R, Kitis O: Conventional and diffusion-weighted MR imaging of intracranial tuberculomas. A case report. Acta Radiol 2002; 43: 560-562.
- Sun WJ, Wang FY: Intrasellar tuberculoma: case report. Chin Med J 2004;117:153-154.
- Domingues FS, de Souza JM, Chagas H, Chimelli L, Vaisman M: Pituitary tuberculoma: an unusual lesion of sellar region. Pituitary 2002; 5: 149-153.
- Freda PU: Tuberculosis of the pituitary and sellar region. Pituitary 2002; 5: 147-148.
- Shahat AH, Rahman NU, Obaideen AM, Ahmed I, Zahman Au A: Cranial-epidural tuberculosis presenting as a scalp swelling. Surg Neurol 2004; 61: 464-466.
- Poonnoose SI, Singh S, Rajshekhar V: Giant cerebellar tuberculoma mimicking a malignant tumour. Neuroradiology. 2004; 46:136-139.
- Ozveren F, Cetin H, Guner A, Kandemir B: Intracranial tuberculoma mimicking metastasis from renal tumor-case report. Neurol Med Chir. 1997;37: 475-478.
|