Abstract
Systemic sclerosis is a systemic inflammatory disorder characterized by the accumulation of collagen and other matrix constituents in the skin and target internal organs. Autoimmune hepatitis with scleroderma is a rare overlapping syndrome. Here we report a 55 year old female patient with coincidence of autoimmune hepatitis, polymyositis and systemic sclerosis.
Keywords :
Collagen
, Polymyositis
, Systemic sclerosis
Turkish Abstract
Sistemik skleroz cilt ve iç organlarda kolajen ve diğer matris bileşenlerinin birikimi ile karakterize sistemik inflamatuar bir hastalıktır. Skleroderma ile otoimmün hepatit birlikteliği nadir görülen bir çakışma sendromudur. Biz burada 55 yaşında skleroderma, otoimmün hepatit ve polimyozit birlikteliği olan vakamızı sunduk.
Turkish Keywords :
, Kolajen
, Polimyozit
, Sistemik skleroz
Introduction
Autoimmune hepatitis (AIH) is an immune-mediated progressive liver disease characterized by autoantibody seropositivity, increased serum immunoglobulin G concentration and interface hepatitis 1. AIH is usually detected during the diagnostic workup of elevated liver enzymes. Classification of AIH is based upon circulating autoantibodies 2. Type 1 AIH is characterized by being positive for anti-nuclear (ANA) and/or anti-smooth muscle antibodies (SMAs) whereas type 2 is defined by the presence of anti-liver kidney microsomal antibody type 1 (LKM-1) and/or anti-liver cytosol type 1 (LC-1) autoantibodies. AIH is associated with connective tissue disease such as Sjogren's syndrome, systemıc lupus erythematosus and mix connetıve tissue disease 3. Systemic sclerosis (SSc) is a connective tissue disease of unknown cause characterized by fibrosis of skin and internal organs. The incidence of gastrointestinal involvement in SSc is 50-90%. In SSc, primary biliary cirrhosis incidence is increased but AIH is observed rarely. Here, we report a rare case of coincidence of AIH, polymyositis(PM) and SSc.
Case Report
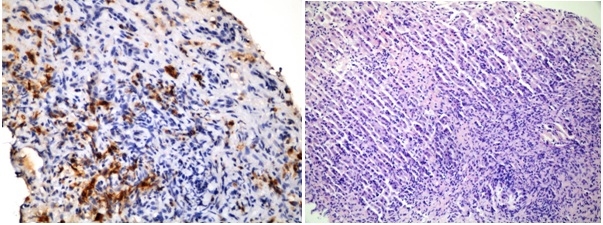
A 55-year-old female patient was admitted with weakness and fatigue. Elevated liver enzymes (ALT 168 IU, AST 126 IU) were detected. Screening for celiac disease, viral hepatitis, steatohepatitis, alpha-1 antitrypsin deficiency, dyslipidemia, Wilson's disease were negatif and hepatotoxic drug usage and alcohol intake was not reported. Liver ultrasonography (USG) was normal. Immunological tests demonstrated positive smooth muscle antibody and positive anti-nuclear antibody with nucleolar staining pattern. Hypergammaglobulinemia with elevated Ig G level (IgG 2200 mg/dl N: 700-1600 mg/dl) was detected. Liver biopsy was performed due to the high suspicion of AIH. Liver biopsy showed plasma cell and lymphocyte infiltration with interface hepatitis and piecemeal necrosis in portal area (Figure 1) .
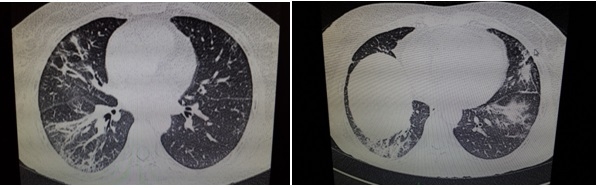
The histological features and immunological tests were consistent with autoimmune hepatitis. She was treated with oral steroid and azathioprine. Her liver enyzmes improved rapidly after corticosteroid treatment. Five years after diagnosis she was admitted with widespread pain throughout the body, progressive muscle weakness developing over months, shortness of breath, dry cough and reduced ability to exercise. Clinical examination revealed symmetric proximal muscle weakness, narrowed mouth orifice, thicken and harden on the hands, face and trunk, bilateral inspiratory rales on pulmonary auscultation . Laboratory and immunological investigations showed: sedimantation 55 mm/h, lactate dehydrogenase 1003 U/L (N:0-247), AST 153 IU(N:0-31), creatine phosphokinase 1588 IU/L (N:0-145), ANA nükleolar patern 3+ with anti PM-SCL 3+. Restrictive ventilatory defect and decreased diffusing capacity for carbon monoxide (DLCO) were demostrated with pulmonary function tests. High-resolution computed tomography (HRCT) showed bibasillary interstitial fibrosis, cystic changes and bronchovascular wall thickening(figure2).
Electromyogram (EMG) findings consistent with myopathy that myofibrils irritation(fibrillation potentials, complex repetitive discharges, positive sharp waves) at rest and short-term, low-amplitude polyphasic contraction were detected. The patient was diagnosed with systemıc sclerosis and probably inflamatory myositis. Treatment with 1 mg/kg/day methylprednisolone was initiated while continuing azathioprine treatment(2 mg/kg/day). Grade 1-2 esophageal varices at endoscopy, granular liver parenchyma, splenomegaly at ultrasound were detected. The patient was considered to be Child-pugh class A cirrhosis. After reduction of steroid doses, increased CPK-AST-LDH values and muscle weakness were observed. As a result of this intravenous immunoglobulin (400 mg / kg / day) was added. Azathioprine was changed to Cyclosporine (3,5 mg/kg/day) to reduce the recurrence. Follow-up showed improvement in the patient's clinical and laboratory values.
Discussion
SSc is a systemic inflammatory disorder characterized by the accumulation of collagen and other matrix constituents in the skin and target internal organs 4. Nearly 90 percent of scleroderma patients have some degree of gastrointestinal involvement. Primary biliary cirrhosis (PBC) is the most common hepatic manifestation 5. PBC is a chronic progressive cholestatic disease leading to cirrhosis. Two studies showed a much higher prevelence of PBC in patients with SSc (approximately 2 percent) than in the general population ( 0.04 percent). Most patients with PBC and SSc have limited cutaneous SSc or overlapping syndromes; diffuse SSc is much less common. Hepatic disease is rare in SSc 5,6. In a study of 262 patients with SSc, 4 patients were confirmed to have chronic liver disease 7. Autoimmune hepatitis (AIH) with scleroderma is a rare overlapping syndrome. AIH is a chronic hepatitis that is characterized by immunologic and autoimmunologic features, generally including the presence of circulating autoantibodies and high serum globulin concentrations. There are 2 types of autoimmune hepatitis. Type 1, classic AIH, is characterized by circulating antibodies to nuclei (ANA) and/or smooth muscle (ASMA). Type 2 AIH is defined by the presence of antibodies to liver/kidney microsomes (ALKM-1) and/or to a liver cytosol antigen (ALC-1) 8-10.
The inflammatory myopathies are rare disorders including polymyositis (PM), dermatomyositis (DM) and autoimmune necrotizing myopaties (NMs). They present acutely, subacutely or chronically with weakness of the proximal muscles, an elevated serum creatine kinase and inflammatory cells on biopsy. The prevalance of myopathies in SSc patients varies from 5-81% 11,12.
We report a case of type 1 AIH, SSc and polymyositis overlap syndrome. AIH was diagnosed by positive ANA, increased serum IgG concentration and histological findings. SSc and polymyositis symptoms began 5 years later. Patients with overlap syndrome were found to increase mortality due to myocardial and pulmonary involvement. For this reason overlap syndromes should be considered when the patient is diagnosed with SSc.
References
- Krawitt EL. Autoimmune hepatitis. N Engl J Med. 2006;354:54.
- Liberal R, et al. Diagnostic criteria of autoimmune hepatitis. Autoimmun Rev. 2014;13(4-5):435-40.
- Manns MP, et al. Diagnosis and management of autoimmune hepatitis. Hepatology. 2010;51:2193.
- Marie I, et al. Autoimmune hepatitis and systemic sclerosis: a new overlap syndrome? Rheumatology (Oxford). 2010;40(1):102-6.
- Assassi S, et al. Primary biliary cirrhosis (PBC). PBC autoantibodies and hepatic parameter abnormalities in a large population of systemic sclerosis patients. J Rheumatol. 2009;36:2250.
- Jacobsen S, et al. Clinical features and serum antinuclear antibodies in 230 Danish patients with systemic sclerosis. Br J Rheumatol. 1998;37:39.
- Abu-Shakra M, Guillemin F, Lee P. Gastrointestinal manifestations of systemic sclerosis. Semin Arthritis Rheum. 1994;24:29-39.
- Toyoda M, et al. Primary biliary cirrhosis- autoimmune hepatitis overlap syndrome concomitant with systemic sclerosis, immune thrombocytopenic purpura. Intern Med. 2009;48(23):2019-23.
- You BC, et al. Liver cirrhosis due to autoimmune hepatitis combined with systemic sclerosis. Korean J Gastroenterol. 2012;59(1):48-52.
- Ishıkawa M, et al. CRST syndrome (calcinosis cutis, Raynaud's phenomenon, sclerodactyly, and telangiectasia) associated with autoimmune hepatitis. Intern Med. 1995;34(1):6-9.
- Pamfil C, et al. Systemic sclerosis-polymyositis overlap syndrome associated with autoimmune hepatitis and cerebral vasculitis. J Gastrointestin Liver Dis. 2012;21(3):317-20.
- Lis-Swiety A, et al. Systemic sclerosis-polymyositis overlap syndrome accompanied by autoimmune hepatitis and sarcoidosis of mediastinal lymph nodes. J Eur Acad Dermatol Venereol. 2006;20(1):107-8.
|