Abstract
Autosomal dominant polycystic kidney disease (ADPKD) is the most common inherited disorder of the kidneys. Approximately 30 to 50 percent of patients with ADPKD will have urinary tract infection during their lifetime. Cyst infections responsible for hospitalization occur much less frequently and which are difficult to treat because many antibiotics do not penetrate the cysts. Infected cysts are a frequent and serious complication of ADPKD. When cysts are not associated with collecting system pyuria is not expected to be seen. This article describes the clinical course of a 51-year-old woman with ADPKD who admitted to the emergency department with fever and abdominal pain developed an infection without pyuria in at least one of the cysts in her kidneys. In conclusion keep in mind that, infected cyst can be seen in patients with ADPKD without pyuria and this situation affects the morbidity of the disease and lead to hospitalization.
Keywords :
Autosomal Dominant Polycystic Kidney Disease
, Cyst infections
, Emergency department
Turkish Abstract
Otozomal dominant polikistik böbrek hastalığı böbreklerin sık görülen kalıtsal hastalıklarından birisidir. Hastaların yaklaşık %30 ila 50'si yaşamları boyunca en az bir kez idrar yolu enfeksiyonu geçirmektedirler. Kist enfeksiyonu geliştiğinde ise yüksek oranda hastaneye yatırılarak tedavi edilmesi gerekir ve birçok antibiyotik, kistlere nüfuz etmediği için tedavisi zordur. Enfekte kistler hastalığın sık ve ciddi bir komplikasyonudur. Kistlerin toplayıcı sistem ile ilişkisi olmadığında piyüri görülmesi beklenmemektedir. Bu makalede, 51 yaşında bilinen otozomal dominant polikistik böbrek hastalığı olan ateş ve karın ağrısı ile acil servise başvuran bir kadın hastada piyüri olmaksızın gelişen kist enfeksiyonu vakası sunulmuştur. Otozomal dominant polikistik böbrek hastalarında piyüri eşlik etmemesine rağmen kist enfeksiyonunun gelişebileceği bilinmelidir. Bu durumun hastalığın morbiditesini etkilediği ve tedavisinin hastanede yatarak olması gereği unutulmamalıdır.
Turkish Keywords :
, Otozomal Dominant Polikistik Böbrek Hastalığı
, Kist enfeksiyonu
, Acil servis
Introduction
Autosomal dominant polycystic kidney disease (ADPKD) is the most common inherited disorder of the kidneys. ADPKD is genetic disorder characterized by the growth of numerous cysts in the kidneys which is a common cause of end-stage renal disease. When cysts form in the kidneys, they are filled with fluid. Cysts can profoundly enlarge the kidneys while replacing much of the normal structure, resulting in reduced kidney function and leading to kidney failure. People with ADPKD tend to have frequent urinary tract infections, which can be treated with antibiotics. People with the disease should seek treatment for urinary tract infections immediately because infection can spread from the urinary tract to the cysts in the kidneys. Cyst infections are difficult to treat because many antibiotics do not penetrate the cysts. Infected cysts are a frequent and serious complication of ADPKD. Approximately 30 to 50 percent of patients with ADPKD will have urinary tract infection during their lifetime. Cyst infections responsible for hospitalization occur much less frequently, approximately 9 percent. An infected cyst and acute pyelonephritis are the most common kidney infections, although complications such as a perinephric abscess and bacteremia can occur 1.
This article describes the clinical course of a 51-year-old woman with ADPKD who admitted to the emergency department with fever and abdominal pain developed an infection without pyuria in at least one of the cysts in her kidneys.
Case Report
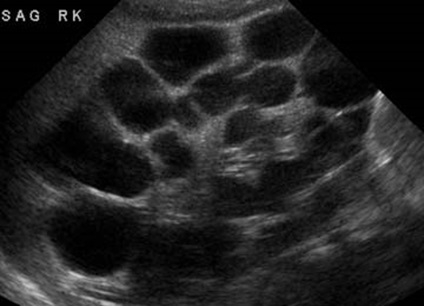
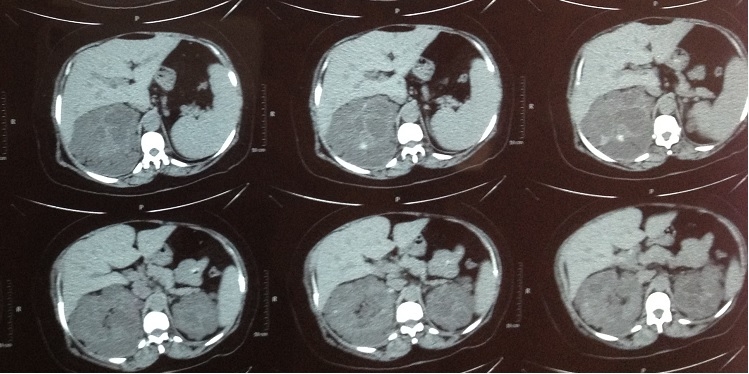
A 51 year old female patient with ADPKD which already showned genetic diagnosis of PKD2 gen mutation, hypertension (HT) and diabetes mellitus (DM) presented to the Emergency Department (ED). She complained with abdominal pain radiating to back and sudden onset of fever. Upon admission to the ED her fever is 38.2°C while her other vital signs were within normal range respectevly blood arteriel pressure was 138/88mmHg, heart rate was 88 beats/minute, respiratory rate was 16/minute. Physical examination revealed distended abdomen, tenderness on palpation and on the left side of the abdomen a palpable mass formation until the pelvic area. Laboratory examination showed that increased white blood count (WBC, 11500/?l), blood urea nitrogen (BUN, 76.6mg/dl), creatinine (Cr, 2.70mg/dl) and C-reactive protein (CRP, 19.16mg/dl) while the other laboratory examinations were within normal range. There was no significant pyuria in urinalysis (leukocyte 3-4/every field). Radiologic exams of the kidney, ureters, and bladder was obtained and showed no evidence of renal stones. Abdominal ultrasonography (USG) confirmed the presence of enlarged kidneys, containing multiple cysts of various sizes; some of the cysts showed internal echo, indicating either cystic hemorrhage or infection. Abdominal computed tomography (CT) was consistent with the suspected infected cyst (Figure 1).
After started intravenous antibiotics and supportive treatment, the patient was transferred to nephrology department with diagnosed renal cyst infection.
Discussion
Cyst infection is a frequent and serious complication of ADPKD, often being difficult to diagnose and treat. Suwabe et al showed that when there was suspected infected cyst WBC >10,000/?l, CRP >15.0mg/dl, and body temperature >38°C strongly suggested cyst infection 2. According to another study to cyst infections was considered as likely in the presence of all of the following features: Fever (temperature >38.5°C for >3 days), abdominal pain (particularly a palpable area of renal or liver tenderness), increased CRP (>50 mg/L), and the absence of any significant recent intracystic bleeding (based on the results of an abdominal CT scan) or other causes of fever 3.
The most common clinical signs of cyst infection is high fever and side pain. In laboratory data, only 45% of cases occur pyuria. As the same, in our case there was no significant pyuria. Cyst infection is likely to be present when the patient experiences an abrupt onset of pain in conjunction with dysuria and frequent fever. Moreover, cyst infection is likely to be present if positive results are obtained from urine cultures testing for the presence of bacteria; however, urine culture results can also be negative for bacteria in patients. This is because many cysts do not communicate with the rest of the urinary tract; thus, a patient with a cyst infection may not experience urinary tract symptoms and bacteriuria.
Radiologic exams (USG, CT), however, do not show signs of infection. Although accurate detection of infected cysts from among the numerous renal cysts present is often difficult, because the findings of infected cysts on CT resemble those of normal cysts. Diffusion-weighted magnetic resonance imaging (DWMRI) is occasionally used in the diagnosis of cerebral abscesses, infected hepatic cysts 4,5. Katano and et al showed that infected renal cysts also was higher signal intensity than normal cysts with DWMRI and they were said, DWMRI was very effective in detecting infected cysts in their patient and may be of value in other such cases with ADPKD 6. However, positron emission tomography (PET) scan will probably make the diagnosis of cyst infections easier and more accurate 7,8. As in Emergency Department, if there is no chance of imaging method, clinician must consider the disease according to symptoms and laboratory data. In our case, although CT showed suspected infected cyst, the clinical findings and laboratory data showed the cyst infection.
References
- Dhamidharka VR. Infected kidney cysts. Kidney Int. 2006;69(5):783.
- Suwabe T, et al. Clinical features of cyst infection and hemorrhage in ADPKD: new diagnostic criteria. Clin Exp Nephrol. 2012;16(6):892-902.
- Sallée M, et al. Cyst infections in patients with autosomal dominant polycystic kidney disease. Clin J Am Soc Nephrol. 2009;4(7):1183-9.
- Ichioka K, et al. A. Diffusion-weighted magnetic resonance imaging of infected renal cysts in a patient with polycystic kidney disease. Urology. 2007;70(6):1219.
- Kita Y, Soda T, Terai A. Diagnosis and localization of infected renal cyst by diffusion-weighted magnetic resonance imaging in polycystic kidney disease. Int J Urol. 2009;16(11): 918-9.
- Katano K, et al. Efficacy of diffusion-weighted magnetic resonance imaging in detecting infected cysts in a case of polycystic kidney disease. Clin Nephrol. 2011 Feb;75 Suppl 1:24-6.
- Jiménez-Bonilla JF, et al. Hepatorenal polycystic disease and fever: diagnostic contribution of gallium citrate Ga 67 scan and fluorine F 18 FDG-PET/CT. Eur Urol. 2011;59(2):297-9.
- Soussan M, et al. Diagnosis and localization of renal cyst infection by 18F-fluorodeoxyglucose PET/CT in polycystic kidney disease. Ann Nucl Med. 2008;22(6):529-31.
Information Presentation
Bu olgu sunumu 19-22 Eylül 2012 tarihlerinde Antalya?da düzenlenen 3. Uluslararası Avrasya Acil Tıp Kongresi (EurAsian2012)?de poster olarak sunulmuştur.
|