Abstract
Lymphangiomatous lesions are most frequently seen in head and neck region, and often located at the cheek, tongue, sublingual region, and hypopharynx. Lymphangiomatous polyps originating from the palatine tonsils are rarely seen. In this report, two female patients, one 12 and the other 56 years old, who were detected to have a mass on the surface of their palatine tonsils which was diagnosed as lymphangiectatic fibrous polyps histopathologically are being presented.
Keywords :
Oropharynx
, Tonsilla palatina
, Fibrovascular polyp
Turkish Abstract
Lenfanjiomatoz lezyonlar, sıklıkla baş-boyun bölgesinde özellikle yanak, dil, sublingual bölge ve hipofarenks yerleşimlidir. Palatin tonsil yerleşimli lenfanjiomatoz polipler oldukça nadir görülmektedir. Bu makalede, tonsilla palatina yerleşimli lenfanjiomatoz fibroz polip tanısı alan 12 ve 56 yaşlarında 2 kadın hasta sunulmuştur.
Turkish Keywords :
, Orofarenks
, Tonsilla Palatina
, Fibrovasküler Polip
Introduction
Lymphangiomatous polyps of palatine tonsils are rarely seen tumor-like benign lesions. Except for a series of 26 cases described by Kardon 1, only a small number of case reports exist, giving a total number of about 50 reported cases 2-8 Histopathologically, these lesions contain mostly lymphatic vessels, as well as varying amounts of fibrous, adipose and lymphoid tissues. Various names have been given to these structures in the literature: lymphangioectatic fibrous polyps, polypoid lymphangiomas, and lymphangioectasic fibrolypomatous polyps, and lymphangiomatous polyps 1-9. The differential diagnosis of a lymphangiomatous polyp includes lymphangiectasia, hemangioma, arteriovenous malformation, juvenile angiofibroma, fibroepithelial and hamartomatous polyps 9-15.
Due to the limited number of cases, a standard treatment approach according to age, sex, and symptomatology has not been determined yet. Symptoms are often vague or are attributed to another disease process, such as chronic or recurrent tonsillopharyngitis. With a careful physical examination however, the abnormal mass on one of the tonsils can be recognized. The polyp was unilateral in all but one case report of bilateral tonsillar lymphangiomatous polyps 8. An accurate diagnosis can be made histopathologically after tonsillectomy or excisional biopsy.
We present two female patients with their decent consent who had a lymphangiomatous polyp of one of her palatine tonsils and review the literature about this condition.
Case Report
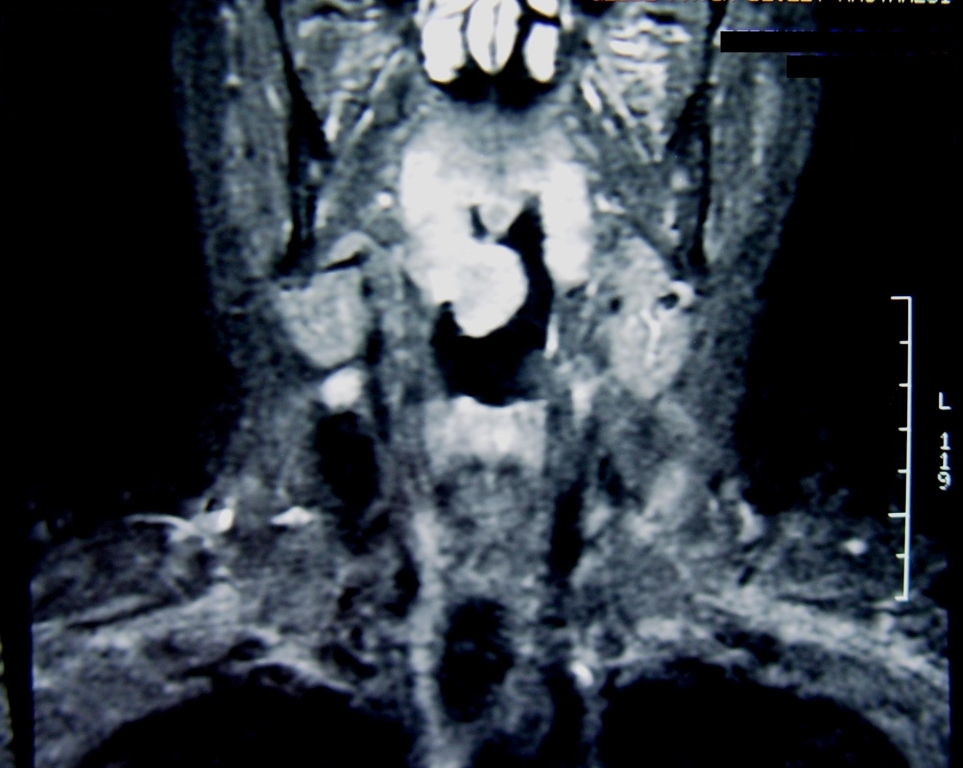
Case 1: A 56-year-old woman presented to our outpatient ENT clinic with a history of progressive difficulty in swallowing and sticking in her throat for 2-3 years. On physical examination, a yellowish-pink mass (2.0 x 1.5 x 1.5 cm) with a smooth surface, rubbery consistency, and wide pedicle was found on the right tonsil. The remainder of the ENT exam was normal, and no lymphadenopathy in the head and neck area was present. MRI showed a polypoid mass on the right tonsil, hyperintense on T2 with peripheral contrast enhancement. The fatty area in between the mass and the surrounding tonsillar tissue was clean (Figure 1).
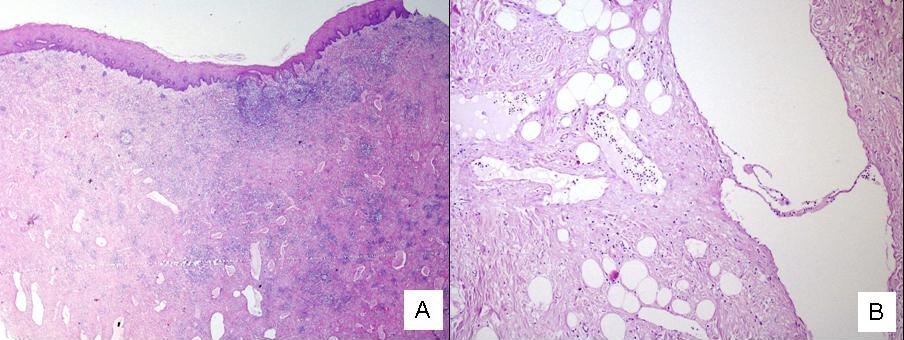
The mass was excised under local anesthesia with wide margins. Macroscopically the polyp?s surface was smooth and its cut surface was white. Microscopic evaluation showed dilated vascular spaces surrounded by a matrix of fibrous connective tissue, lymphoid aggregates, and scattered adipose tissue. The adipose tissue was mainly found in the upper part of the lesion along with lymphoid tissue. The mucosal surface was covered by squamous epithelium, with no hyperplastic or dysplastic changes. The final histopathologic diagnosis was a lymphangiomatous fibrous polyp. The surgical margins were found to be clean in the excision specimen (Figure 2).
Case 2: After presenting to various physicians 7-8 times over the previous year with complaints of a sore throat, a ten-year old girl was directed to our clinic by an ENT specialist after he visualized a mass in her oropharynx. On physical examination, we detected a greyish-yellow colored hard mass (1.5 x 1.5 x 1.0 cm) which was connected to the central area of the right tonsil by a wide pedicle (Figure 3).
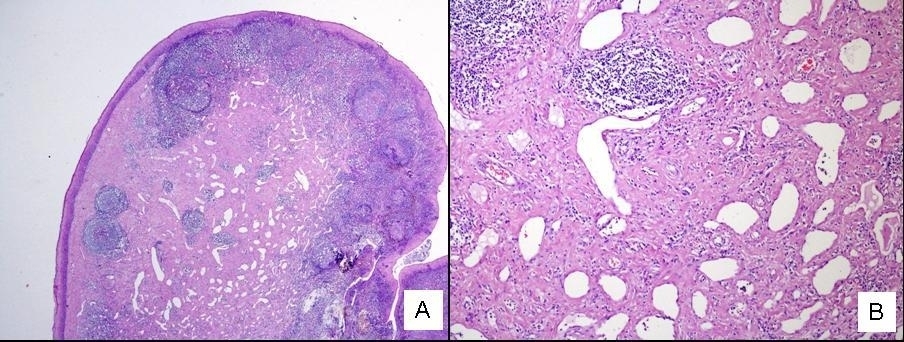
The left tonsil was normal in size and appearance. Upon neck palpation, upper cervical jugulodigastric lymphadenopathy (1.5 x 1.5 cm) was found bilaterally. MRI showed a mass lesion on the right tonsil (1.5 x 1.5 x 1.0 cm) which was hyperintense compared to the surrounding tonsillar tissue and showed peripheral contrast enhancement on T2 sequences. Under general anesthesia, the mass on the right tonsil was excised. Histopathologically, the polyp showed dilated lymphatic channels surrounded by fibrous tissue and remnants of lymphoid tissue covered by stratified squamous epithelium. The mass was diagnosed as a lymphangiomatous fibrous polyp of the tonsil. The surgical margins in the specimen were clean (Figure 4).
Immunohistochemical studies were not performed in our patients. On follow-up 6, 12, and 24 months later (case 1) and 10 months later (case 2), throat examination was normal.
Discussion
More than 90% of the lymphangiomatous lesions are localized in the head and neck region, most frequently in the cheek, tongue, sublingual and hypopharyngeal areas, and less often at the larynx or parotid gland 16. Lymphangiomatous lesions are very rarely seen in the palatine tonsils. Hyams reports that 8% of benign tonsillar lesions are lymphangiomatous 9. Kardon, in his large series (n=26), mentioned that lymphangiomatous polyps (LP) constituted 1.9% of all tonsillar tumors 1. Chen summarized 30 published cases of LP and made the first report of a patient with bilateral LP 8. The large series of palatine tonsils LP cases reported by Kardon were collected over a period of 19 years 1. In this report, just two palatine tonsils LP cases who were detected in our clinic over a 15-year time span are described. In the cases described in the literature, male:female prevalence was about equal and ages of the cases was from 3- to 63-years old 1-8.
The clinical features of the palatine tonsils LPs are often non-specific. Early in the course, vague complaints associated with the throat may be felt as the oropharyngeal mass slowly grows. Patients may complain of chronic or recurrent sore throat, difficulty in swallowing, a ?stuck? feeling in the throat, etc. Swallowing and respiratory complaints may arise as the mass enlarges. They are often detected incidentally during a physical examination of the throat 1-8. Such was the presentation (sore throat and ?stuck? feeling in the throat) in both of our patients, which led to the discover of the LP on physical examination.
Lymphangiomatous polyps of the palatine tonsils are benign lesions, generally assumed to be hamartomatous in nature. The histogenesis is unclear, but these lesions are thought to be hamartomatous because they consist of a haphazard proliferation of elements that are found in normal tonsillar tissue. Based on these findings, LPs, including the ones in this report, are non-neoplastic rather than truly neoplastic. Their pathogenesis may involve inflammatory obstruction to lymphatic channels leading to lypmhangiectasia and edema 12-15.
Macroscopically, palatine tonsil LPs range in size from 0.5 cm to 3.8 cm (mean 1.6 cm) 1-8, which is the range of those described here (1.5 and 2.0 cm). Lesions described in the literature were pedunculated, polypoid, or sessile masses arising from the surface of the tonsil without showing any infiltration of the underlying stroma. They were usually described as polypoid with a smooth white, tan, or yellow cut surface, and some were partially bilobed. Regarding firmness, the masses varied from spongy to firm and fibrous. Histological examination typically revealed a polypoid mass composed of dilated, thin-walled lymphatic channels filled with pale eosinophilic fluid containing intraluminal lymphocytes, and embedded in loose or more dense fibrovascular stroma. The surrounding tonsillar lymphoid tissue was compressed but histologically normal and the entire mass was covered by a thick layer of stratified squamous epithelium. Scattered randomly throughout the fibrovascular stroma were variable numbers of lymphocytes, which in some instances showed follicle formation. Inside the lesion was scattered fatty tissue, mainly found in the upper part of the along with lymphoid tissue. The reason of fatty tissue is ischemic changes as a result of degeneration or tissue metaplasia during the long clinical course, as in case 1, whose complaints began two years prior to presentation. In the second case, no fatty tissue was seen. The diagnosis of such lesions does not require ancillary tests, but researchers have found the endothelial tissue of these lesions to be immunologically reactive for factor VIII-related antigens, anti-CD31, and anti-CD34, and lymphocytes reactive for CD4 5RB[LCA], CD3 [T-cell] and CD20 [B-cell] 1-8.
The differential diagnosis of a polypoid lesion includes neoplastic and non-neoplastic conditions such as an inflammatory polyp, lipoma, hemangioma, lymphangioma, schwannoma, lymphangiectasia, arteriovenous malformation, juvenile nasopharyngeal angiofibroma, fibroepithelial polyp, and a pedunculated squamous papilloma 13,15. Over time, fatty content in a particular tissue might increase, as in a lipoma or fibrolipoma. If lymphatic or blood vessels predominate, terms such as lymphangioma, lymphangiectatic fibrolipomatous polyp, and lymphangiomatous polyp are used to describe the lesion 15. Especially in male adolescents, juvenile nasopharyngeal angiofibroma should be ruled out and treated aggressively if present, as they can become very large, eroding into bone and causing severe epistaxis due to their rich blood supply. Histologically, angiofibromas have a more cellular stroma, with stellate and plump cells, along with staghorn-like thin vascular channels while the LPs contain varying amounts of lymphoid infiltrate, adipose tissue, fibrous tissue and dilated vessels 1,14. Unlike in a pedunculated squamous papilloma, the squamous epithelium of an LP is not a proliferative component, but rather a lymphatic and lymphocytic component 15. Kardon prefered the term lymphangiomatous polyp rather than lymphangioma for these lesions because their pathogenesis was still unclear 1. As noted in the literature, the lymphatic channels of LPs are frequently dilated, but not usually as prominent as in a typical lymphangioma. In addition, the stromal components of LPs are usually more abundant than vasculature 1.
Regarding treatment of LPs located on the tonsils, most authors report performance of a tonsillectomy for the patients. In our patients however, local excision from the tonsillar surface was performed with safe margins and no complications. No recurrence was seen after 2 years in one patient and 10 months in the other patient.
Conclusion
Lymphangiomatous polyps of palatine tonsils which can be treated by local excision from the tonsillar surface are rarely seen tumor-like benign lesions.
References
- Kardon DE, Wenig BM, Heffner DK, Thompson LD. Tonsillar lymphangiomatous polyps: a clinicopathologic series of 26 cases. Mod Pathol. 2000; 13: 1128-33.
- Hiraide F, Inouye T, Tanaka E. Lymphangiectatic fibrous polyp of the palatine. J Laryngol Otol. 1985; 99: 403-9.
- Al-Samarrae SM, Amr SS, Hyams VJ. Polypoid lymphangioma of the tonsil: report of two cases and review of the literature. J Laryngol Otol. 1985; 99: 819-23.
- Sah SP, Bahadur KC, Rani S. Lymphangiectatic fibrolipomatous polyp of the palatine tonsil. Indian J Pathol Microbiol. 2000; 43: 449-51.
- Kühnemund M, Wemert N, Gevensleben H, Gerstner AO. Tonsillar lymphangiomatous polyp. HNO. 2010; 58: 409-12.
- Roth M. Lymphangiomatous polyp of the palatine tonsil. Otolaryngol Head Neck Surg. 1996; 115: 172-3.
- Krausen Ch, Becker K, Hamann KF. Angiofibrolipoma of the tonsil. Laryngol Rhinol Otol. 1986; 65: 355-6.
- Chen HH, Lovell MA, Chan KH. Bilateral lymphangiomatous polyps of the palatine tonsils. Int J Pediatr Otorhinolaryngol. 2010; 74: 87-8.
- Hyams VJ. Differential diagnosis of neoplasia of palatine tonsil. Clin Otolaryngol Allied Sci. 1978; 3: 117-26.
- Borges A, Bikhazi H, Wensel JP. Giant fibrovascular polyp of oropharynx. Am J Neuroradiol. 1999; 20: 1979-82.
- Raha O, Singh V, Purkayastha P. Lymphangioma tonsil ? rare case study. Indian J Otolaryngol Head Neck Surg. 2005; 57: 332?4.
- Shara KA, Al-Muhana AA, Al-Shennawy M. Hamartomatous tonsillar polyp. J Laryngol Otol. 1991; 105: 1089-1090.
- Lupovitch A, Salama D, Batmanghelichi O. Benign hamartomatous polyp of the palatine tonsil. J Laryngol Otol. 1993; 107: 1073-5.
- Duggal P, Chakravotry S, Sharma S, Ahluwalia RK. Peduculated hamartomatous polyp of tonsil in a child; A new presentation. Int J Pediatr Otorhinolaryngol Extra. 2008; 3: 120-3.
- Ohtsuki Y, et al. A peduculated hamartomatous polyp of the palatine tonsil. Biomed Res. 2006; 17: 155-8.
- Stal S, Hamilton S, Spira M. Hemangiomas, lymphangiomas, and vascular malformations of the head and neck. Otolaryngol Clin North Am. 1986; 19: 769-796.
|