Abstract
Three-dimensional transesophageal echocardiography is much better diagnostic tool to conclusively recognize the identification of the anatomy and the abnormalities of the heart valves. In this case report, we tried to emphasize the importance of 3-dimensional transesophageal echocardiography to describe the lesion in the case of infective endocarditis developing on bicuspid aortic valve in a 21-year-old male patient without any cardiovascular disease history, which admitted to hospital with complaint of dyspnea and fever.
Keywords :
Bicuspid aortic valve
, Infective endocarditis
, 3D trasesophageal echocardiography
Turkish Abstract
Kalp kapaklarının anatomisinin ve anomalilerinin belirlenmesi için kullanılan üç boyutlu transözefagiyal ekokardiyografi, diğer görüntüleme tekniği olan transtorasik ekokardiografiden daha üstün bir tanı aracıdır. Bu yazımızda daha öncesinde herhangi bir kardiovasküler hastalık öyküsü olmayan, dispne ve yüksek ateş ile hastanemize başvuran 21 yaşındaki erkek hastada biküspit aort kapak zemininde gelişen infektif endokardit tanısının konmasında üç boyutlu transözefagiyal ekokardiyografinin önemini vurgulamaya çalıştık.
Turkish Keywords :
, Biküspid aort kapak
, İnfektif endokardit
, 3B transözefagiyal ekokardiyografi
Introduction
The bicuspid aortic valve (BAV) is a common congenital cardiac anomaly. The BAV may function normally throughout life, and usually unobserved until valve stenosis or regurgitation appears 1. Furthermore, the BAV is a potential substrate for infective endocarditis (IE), especially in young male patients. The risk of developing IE on a BAV is 10-30% over a lifetime 1. Staphylococci (12% coagulase negative) 2 and viridans streptococci accounted for nearly three-quarters of the cases of IE affecting BAVs 3. Most patients necessitate surgery, frequently on a emergency basis. Rather than transthoracic echocardiography (TTE), transesophageal echocardiography (TEE) plays a critical role in diagnosis and addressing the patient to cardiac surgery 4. In this case report, we tried to emphasize the importance of 3-dimensional TEE to describe the lesion in the case of infective endocarditis developing on bicuspid aortic valve.
Case Report
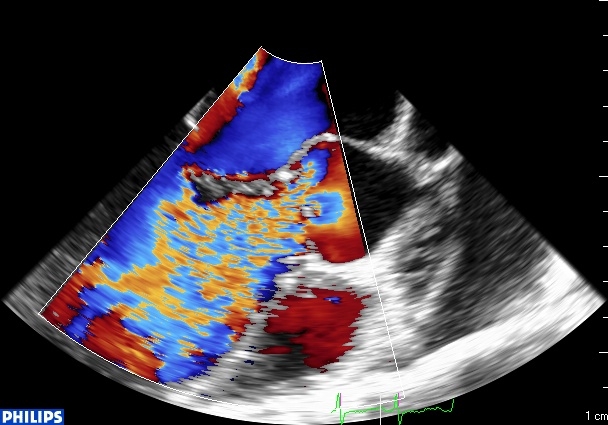
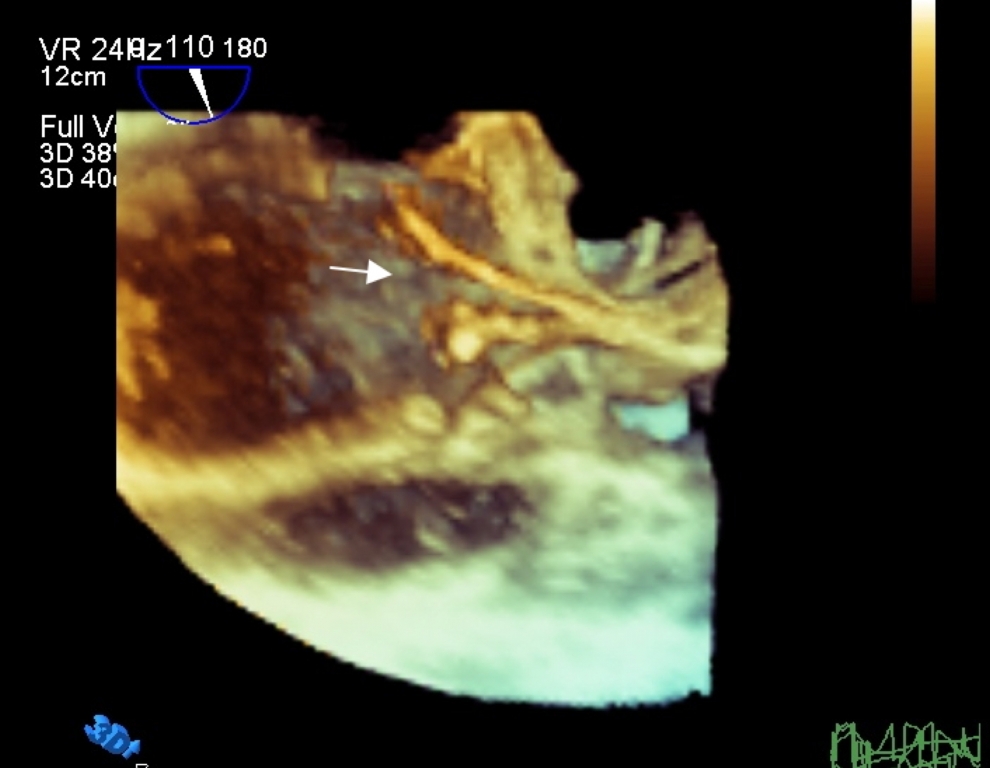
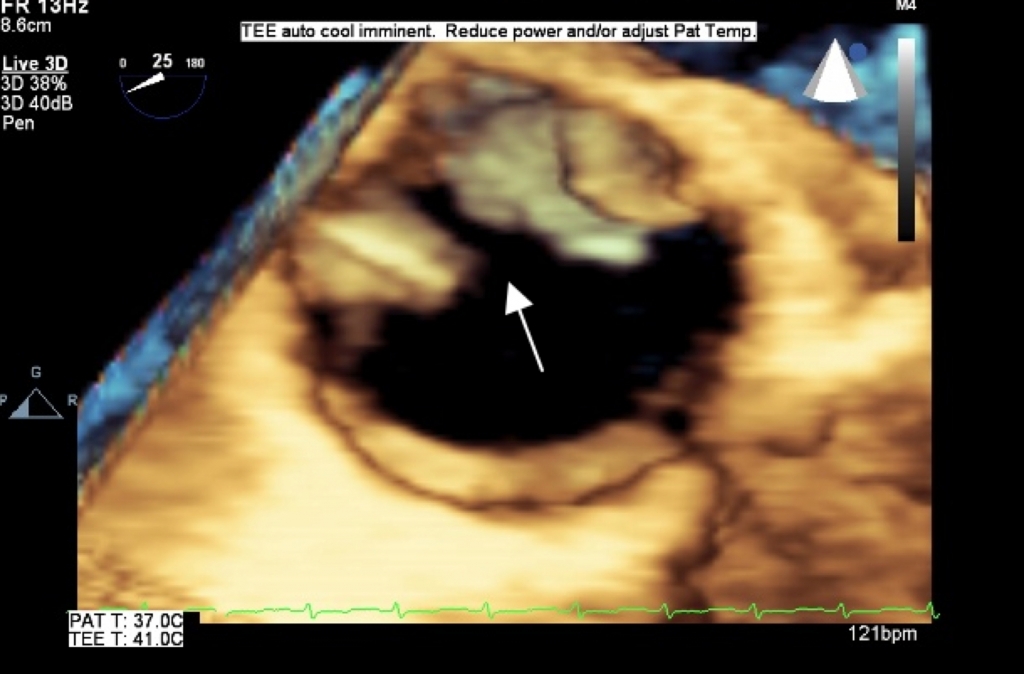
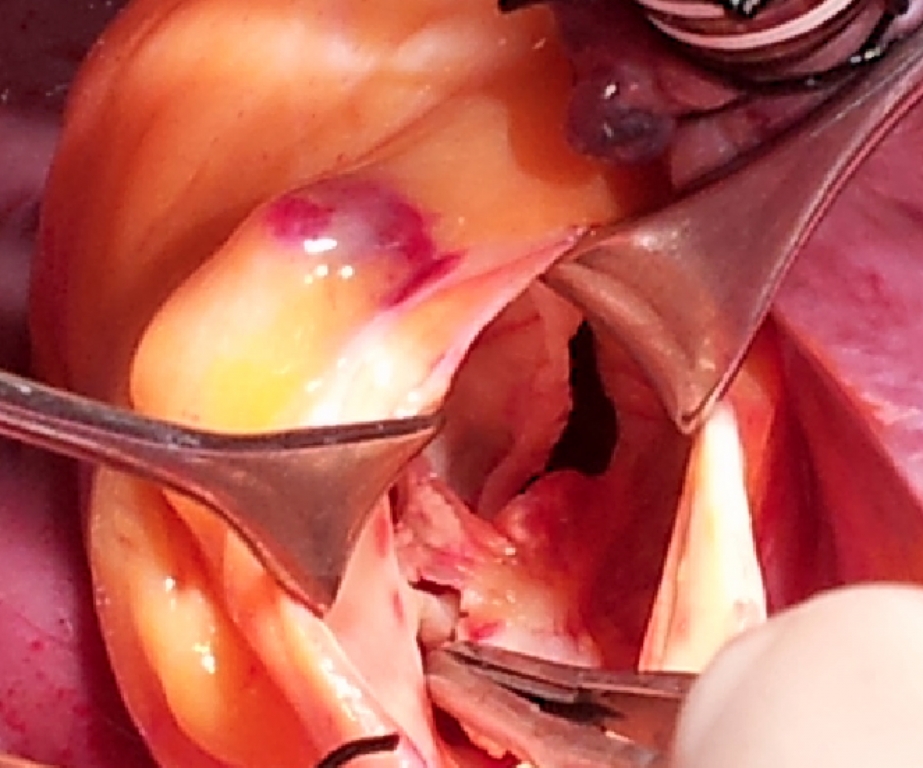
A 21-year-old male patient without any history of cardiovascular disease was admitted to our hospital for dyspnea and fever (?39°C). He had moderate dyspnea (New York Heart Association functional class III). On his physical examination, orthopnea, tachycardia (118/min), roughed lung sounds, and aortic 2-3/4 diastolic murmur were present. We suspected IE with the present findings. Blood and urine cultures were obtained, and then wide-spectrum antibiotherapy was started. TTE examination revealed a severe aortic regurgitation, bicuspid aortic valve with suspected vegetation. In addition to elucidate the findings of 2D TTE, 3D TEE was performed and provided additional information. To clarify this pathology, 3D-TEE was carried out and precisely delineated the lesion by showing a major perforation in the anterior aortic cusp of the BAV. Patient underwent then aortic valve replacement. Intraoperative examination of the aortic valve confirmed the findings of the 3D TEE. (Figure 1A-D)
Discussion
The 3D spatial structure of normal aortic valve is more intricate than known. With the initiation of 3D TEE, a more reliable assessment (superior spatial resolution) of aortic valve can be provided with a good quality than that obtained by 2D TEE alone 5,6. Nonetheless, in the assessment of aortic valve endocarditis, 3D TEE provides invaluable morphological information regarding the define the size, shape, mobility and insertion of vegetation, the extent of leaflet involvement (aneurysms, perforations), annulus and surrounding structures in comparison with 2D TEE 7.
Although 2D TTE and TEE are the conventional procedures for the diagnosis of valvular heart disease, 3D TEE is a better noninvasive tool to define more accurately the intracardiac anatomy. In our case, the images that we obtained with the use of 3D TEE helped us to conclusively recognize the identification of perforation on BAV. In conclusion, 3D TEE should be the method of choice when a definite diagnosis can not be made by 2D TTE or TEE in case of infective endocarditis.
References
- Fedak PW, et al. Clinical and pathophysiological implications of a bicuspid aortic valve. Circulation. 2002;106 (8):900-4.
- Lamas CC, Eykyn SJ. Bicuspid aortic valve--A silent danger: analysis of 50 cases of infective endocarditis. Clin Infect Dis. 2000;30 (2):336-41.
- Hori D, et al. Surgically treated infective endocarditis involving the aortic bicuspid valve and ventricular septum revealing aortic regurgitation and a Gerbode defect. Gen Thorac Cardiovasc Surg. 2010;58 (5):255-9.
- Malagoli A, Barbieri A, Modena MG. Bicuspid aortic valve regurgitation: quantification of anatomic regurgitant orifice area by 3D transesophageal echocardiography reconstruction. Echocardiography 2008;25 (7):797-8.
- Anwar A, McGhie J, Meijboom F, Cate F. Double orifice mitral valve by real time three-dimensional echocardiography. Eur J Echocardiogr. 2008; 9: 731?732.
- Lu Q, Lu X, Xie M, Wang X, Wang J, Yang Y. Real-time three-dimensional echocardiography in assessment of congenital double orifice mitral valve. J Huazhong Univ Sci Technolog Med Sci. 2006; 26: 625?628
- Muraru D, Badano LP, Vannan M, Iliceto S. Assessment of aortic valve complex by three-dimensional echocardiography: a framework for its effective application in clinical practice. Eur Heart J Cardiovasc Imaging. 2012 Jul;13(7):541-55
|