Abstract
Penile duplication (also known as Diphallia or diphallasparatus) and pseudoduplication are rare malformations with an estimated frequency of one case per five million births.
It is commonly associated with duplications or other malformations of the urinary tract, anorectal and vertebral malformations. The embryologic basis of these anomalies is not clearly known.
15-year-old boy presented with the complaint of having two penises. Other external genitalia was normal, two normally positioned testicles within scrotum. He also had a patent anus.
MRI has been used rarely in the imaging of congenital penile abnormalities but has the potential for depicting the abnormal anatomy in planning of reconstructive surgery.
Penile duplication poses a difficult treatment problem in terms of medical, ethical, and aesthetic decision making.
Keywords :
Fluoroscopy
, MR-Imaging
, Ultrasound-Spectral Doppler
, Genital/Reproductive
, Penis
Turkish Abstract
Penil duplikasyon(diğer adıyla Diphallia veya diphallasparatus) beş milyon da bir görülen nadir bir malformationdur. Sıklıkla anorektal, üriner ve vertebral anomalilerle birliktedir.
Hastanemiz üroloji kliniğine penil şekil bozukluğu şikayetiyle başvuran 15 yaşında erkek hasta anomalinin ve eşlik edebilecek diğer patolojilerin görüntülenebilmesi amacıyla radyoloji ünitesine gönderilmişti. MR incelemede tam olmayan psödoduplikasyon ile uyumlu olan ve diğer kanal ile birleşen ikinci bir uretra distalde aksesuar glans düzeyinde künt olarak sonlanmaktaydı. Doppler USG inceleme ile korpus kavernozum ve korpus spongiozum düzeylerinde vasküler yapılar değerlendirildi.
Nadir rastlanan penil duplikasyon olgumuzda yapılan MR , sonografi ve indirekt röntgen incelemelerinin sonuçlarını literatürde rastlanan az sayıda benzer olguları da gözden geçirerek sunmayı amaçladık.
Turkish Keywords :
, Floroskopi
, MR görüntüleme
, Ultrason Spektral Doppler
, Genital / Üreme
, Penis
Introduction
Penile duplication (also known as Diphallia or diphallasparatus) is a rare malformation with an estimated frequency of one case per five million births and is commonly associated with duplications or malformations of the urinary tract, anorectal and vertebral malformations. The embryologic basis of these anomalies is not clearly known. Every case in literature was unique. So, treatment should always be individualized according to the degree of penile duplication and the extent of the concommitant anomalies.
Case Report
Our patient was referred to our magnetic resonance imaging (MRI) unit by examining urologist. After precise sectional study of abdomen and perineum with MRI, looking for possible accompanying genitourinary, gastrointestinal, vertebral and skeletal malformations we also performed retrograde urethrogram and penile duplex sonography. All of these investigations were accomplished with detailed informed consent of patient.
In 1.5 Tesla MRI unit(GE Signa HDX 1.5 T) , 8 channel body array coil was used. Other parameters were FOV: 24 cm, slice thickness: 3 mm ; interval: 0.5 mm; frequency: 320; phase encoding: 256 İn B-mode and duplex sonography, GE Logic 9 and 12 MHertz linear probe was used in order to identify the superficial soft tissue and thin vasculature optimally.
Flouroscopic examination was performed using Toshiba winscope fluoroscopy x-ray machine. Nonionic iodine-contrast medium was injected with no side effects.
We searched published studies using Google academic, Pubmed and reviewed earlier reports similar to our case in the literature published in previous 60 years.
A 15-year-old boy presented with duplication of the penis(Figure 1) , normal scrotum, two descendedtesticles, and a patent normally positionedanus.
The right-sided penis was smallerbut appeared anatomically normal with a smaller glans. Patient said that he was only urinating through the left sided larger penis.
He also reported that erection happens normally but there has been only left-sided ejaculation.
Abdominal ultrasound was normal. Abdominal MRI revealed no gastrointestinal or genitourinary anomalies. There was one urinary bladder opening toward centrally located urethra. Pelvic bones were anatomically intact. Anal canal was patent without any fistulae formation. Urination was through the only patent urethra .
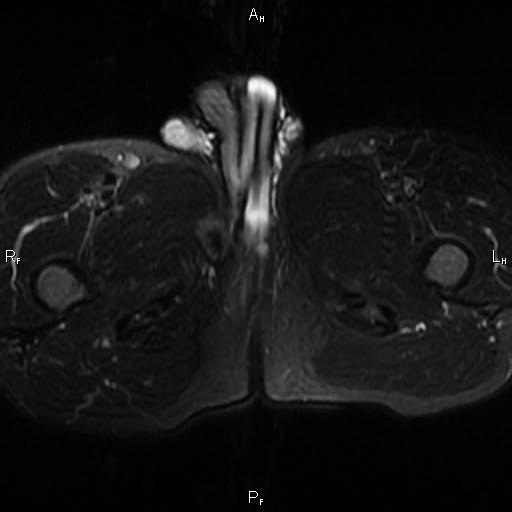
On MRI of perineum and penis the left sided component had a pair of corpora cavernosa- but right one getting thinner after bifurcation- and one corpus spongiosum (Figure 2).
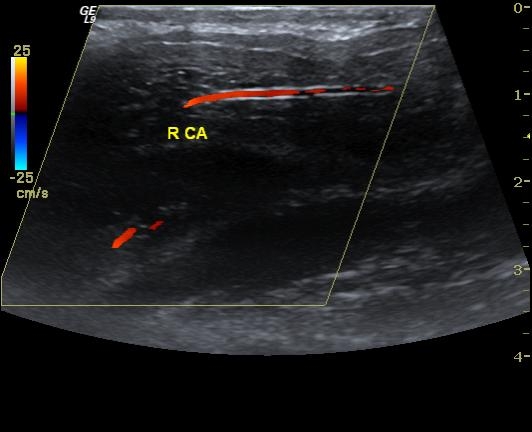
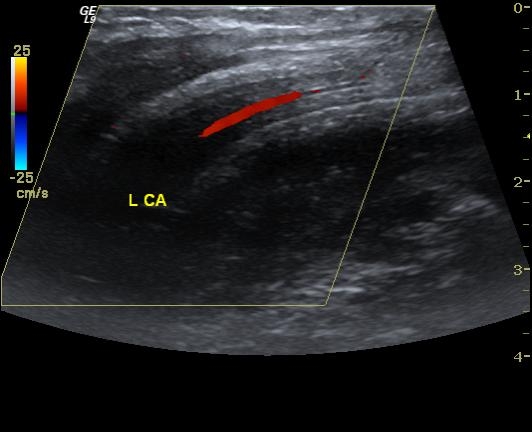
Urethra was tracking normally through spongiose body in the middle. At penile base there were 2 cavernosa and one spongioum. On the right side, cavernous body was split proximally giving rise to larger lateral corpus cavernosum which forms right-sided penile shaft and medial thinner part coursing through the left-sided normal appearing penile shaft(Figure 3). On the right-side there also was a corpus-like structure possibly a rudimentary spongiose component . On duplex Doppler examination cavernosal artery diameter was smaller compared with other side but had similar flow pattern(Figures 4 and 5 ).
We performed retrograde urethrogram-not shown- to define if the rudimentary glans had an real external urethral opening or just a cleft in the tip. Distal opening couldn't be cannulised and happened to be a pseudourethral opening.
Discussion
Diphallia is a rare congenital anomaly. The extent of duplication and the number of accompanying anomalies vary from a double glans arising from a common shaft to complete duplication of the phallus accompanied by multiple anomalies such as bladder exstrophy, colonic duplications, separation of the symphysis pubis and rectus abdominis musculature, neural tube defects and anorectal malformation 1,2.
However, the full constellation of anomalies has rarely manifested in a single case 3. İn literature reported number of cases have been less than 100 and every different case have been unique 1,2.
In some cases, each phallus has only one corporal body and urethra; in others, each phallus has two cavernosal bodies and one urethra. The estimated incidence is about 1 in 5 million live births 1. The first case of diphallus was reported by Wecker in 1609 from a cadaver in Bologna 1.
Embryologically a diphallus deformity is believed to arise from either "separation" of the pubic tubercles, wherein each phallus will have only one corporal body and urethra, or "cleavage" of the pubic tubercle wherein each phallus will have two corporal cavernosus bodies and urethras.
In one case report published in 2004, Bajpai and collegues propose a spectrum of anomalies quoted as one type of incomplete separation of monozygotic twins. These authors claimed caudal twining as the mechanism behind the syndrome. Caudal duplication and consequences were also reported by Ravitch(1953), Hollowel(1977) and Azmy(1990) with larger number of components 3,4.
Caudal duplication syndrome has been proposed to explain the concomitant duplication of hindgut, bladder, and urethra 2. Sarin et al. reported a child with triplication of colon, double bladder, and urethra with diphallus and an umbilical hernia 4. Diphallus has been suggested to arise from failure of fusion of mesodermal bands or presentation of the opportunity for mesoderm to surround 2 urethral anlage by Hollowell 5.
Schneider divided this embryological defect of the penis into three groups: diphallia of the glans alone, bifid diphallia, and complete diphallia 7.
We believe that our case represents a bifid incomplete diphallus(Pseudodiphalli) with incomplete collateral duplication of urethra, corpora cavernous and corpus spongiosum.
The extent of duplication and the range of associated anomalies, usually from the urogenital, gastrointestinal, and musculoskeletal systems, vary significantly.
Intestinal anomalies are mostly associated with complete diphallia, of which imperforate anus and rectoperineal fistula being the most common 8. The urethra shows a range of variations. The meatus may be normal, hypospadiac, or epispadiac, and the scrotum may be normal or bifid.
Therefore, evaluation should include imaging of at least the entire urinary tract. Although ultrasound has been reported to aid in presurgical assessment of the extent of phallic development, MRI has been shown to be extremely helpful in delineating the exact internal anatomy and extent of duplication of corpora and the urethra 9,10.
Penile duplication poses a difficult treatment problem in terms of medical, ethical, and aesthetic decision making. The detailed pelvic anatomy rendered by MRI may therefore increase a surgeon?s understanding of the complex anomalous structures and formulate the most optimal management plan 8.
Although our patient claimed to have no erectile dysfunction it is uncommon for bifid phallic component to erect because of lack of complete neuromuscular development. Reported earlier studies 9 also confirmed that pseudodiphallia is rarely associated with normal function of the rudimentary phallus. We believe this misleading was because of the individual?s embarrassment over the malformation.
Every kind of genital malformation like penile duplication poses a difficult treatment problem in terms of medical, ethical, and aesthetic decision making. Every case in literature has unique components. So, treatment should always be individualized according to the degree of penile duplication and the extent of the concommitant anomalies.
Radiologic methods and especially MRI with multiplanar and high soft tissue resolution helps to identify the extent of the problem.
References
- Mukunda R, Bendre PS, Redkar JG, Hambarde S. Diphallus with anorectal malformation-case report. J Pediatr Surg. 2010; 45: 632?4.
- Bajpai M, Das K, Gupta AK. Caudal duplication syndrome: More evidence for theory of caudal twinning. J Pediatr Surg. 2004;39:223-6.
- Keckler S. Isolated diphallia: Case report and literature review. Eur J Pediatr Surg. 2009; 19: 254?5.
- Sarin YK, Manchanda V, Sharma A, Singhal A. Triplication of colon with diphallus and complete duplication of bladder and urethra. J Pediatr Surg. 2006; 41:1924?6.
- Hollowell JG, et al. Embryologic considerations of diphallus and associated anomalies. J Urol. 1977; 117:728-32.
- Priyadarshi S. Diphallus with ectopic bowel segment: a case report. Pediatr Surg Int. 2005; 21: 681?3.
- Dewan P A, Lawrence M J, Pip A, Kasa S. Diphallus associated with partial caudal duplication. Pediatr Surg Int. 1998: 14: 131-3.
- Wilkins C J, Sriprasad S, Sidhu PS. Colour Doppler ultrasound of the penis. Clin Radiol. 2003; 58: 514?23.
- Gyftopoulus K, Wolffenbuttel KP, Nijman RJ. Clinical and embryologic aspects of penile duplications and associated anomalies. Urology. 2002; 60: 675-9.
- Vossough A, et al. Magnetic resonance imaging of the penis. Abdom Imaging. 2002: 27:640?659.
Information Presentation
This case was presented as e-poster in 17th annual meeting of Turkish Magnetic Resonance Society on May 24-26th 2012, Ankara
|