Abstract
The rupture risk of abdominal aortic aneurysm (AAA) is primarily proportional to the amounth of increase in diameter.In the literatüre ruptured dissected AAA with maximus diameter >13cm is rarely reported and the overall mean age is 70 years.In this article 15 cm in diameter and 59 years old hypertansive male patent with ruptured AAA was presented with the clinical and operative tecniques. The huge size of AAA trumphs the surgical tecniques but meanwhile sometimes the only available treatment is open repair with succesful results. Also in some emergency cases the patient is not stable enough to prepare the preoperative imagining. Our case report describes the giant AAA which presented with rupture and rarely reported.
Keywords :
Abdominal aorta
, Aneurysm
, Rupture
Turkish Abstract
Abdominal aort anevrizmalar (AAA)?da rüptür riski, öncelikle çapları ve artış miktarı ile orantılıdır. Literatürde rüptüre- diseke AAA?larda maksimum çapı >13 cm çok az vaka bildirilmiştir ve genel yaş ortalaması 70 yaş üzeridir. Çapları büyük olan AAA?larda cerrahi yaklaşım çok zor olmaktadır. Bazı durumlarda uygulanabilir tek tedavi şekli , başarılı sonuçları ile açık cerrahi anevrizma tamiri ve operasyonu olmaktadır. Ayrıca, bazı acil durumlarda operasyon öncesi dönemde, görüntüleme tekniklerinin uygulanması için hasta yeteri kadar stabil olmamaktadır. Bu yazıda, 15 cm çaplı rüptüre dev AAA?sı olan 59 yaşındaki hipertansif erkek hasta klinik yaklaşımı ve operasyon teknikleri ile sunulmuştur.
Turkish Keywords :
, Abdominal aort
, Anevrizma
, Rüptür
Introduction
Relation between abdominal aortic aneurysm (AAA) rupture risk and diameter is significant and universally indicated. The data suggest that %20-40 rupture risk for 7-8 cm maximum diameter; and %30-50 of rupture risk for > 9 cm in maximum diameter. In emergency situations of rupture, open repair is the only available operation in most centers. The literature is also presented technical and operative difficulties associated with giant AAAs.
Case Report
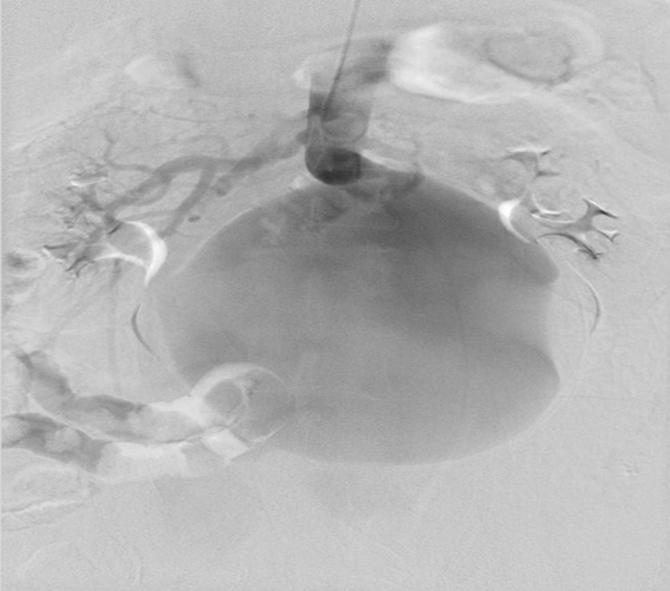
A 59-year-old male was admitted to cardiology unit with chest pain and had planned coronary angiography. Echocardiography documented severe left ventricular hypertrophy, 60% ejection fraction, 1+ functional mitral regurgitation. Overweight patients (111kg) physical examination demonstrated pulsatile machinery murmur and palpable tender abdominal mass in mesogastrium. The angiography showed 50% circumflex coronary artery stenosis and infrarenal giant dissected and ruptured abdominal aneurysm of 13x15 cm (Figure 1). He was transferred to ICU unit from angiography unit. He was heamodynamically unstable with a blood pressure of 175/95 mmHg and a heart rate of 105 beats/min. In the hemogram; hemoglobin was 7.5 mg/dL.
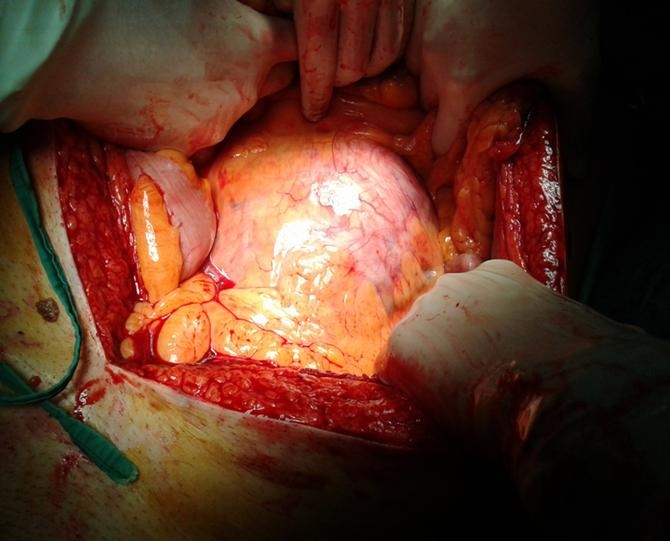
The patient had already taken anticoagulant treatment (4x75 mg klopidogrel peroral, 1x100 mg aspirin peroral and 2x0.6 cc enoxaparin subcutaneous). The aneurysm was not suitable to endovascular treatment because of its proximal neck was < 1 cm to the renal arteries. There was not enough time for a pre-operative diagnosis to be made. He has taken to Operation Theater immediately. A standard midline operative approach was made and before heparin administration (1mg.kg), a giant infra-renal abdominal aortic aneurysm was identified (Figure 2).
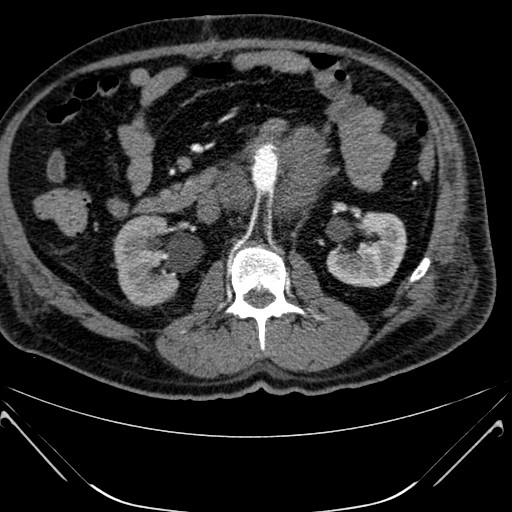
During the operation because of the mass we couldn?t place an X-clamp on the proximal of the neck. By comparison on aorta we made an aortotomy and then place a Foley catheter and fill it with saline solution; by this method, we clamp the aorta and anastomoses, a bifurcated aorto-bifemoral graft (18-9 mm Dacron graft) was sewn end-to-end to the proximal neck, end-to-side to bilateral common femoral artery. Peroperatuarly, we transfused 5 erythrocyte cell packages and 7 fresh frozen plasmas. 10 mg.kg/min dopamine and dobutamine infusion had continued during perioperative period. Intensive care unit stay was 2 days. The patient had an uneventful postoperative course (Figure 3-4) and was discharged home 6 days after the operation with 2x50 mg peroral beta blocker and 1x100 mg aspirin medical therapy.
Discussion
It has been documented that AAAs do not adapt to the Laplace law and can be ruptured at any size. 1-2 Aneurysm rupture involves a complex series of biological changes in the aortic wall3. There is a few literature with a maximum diameter >13 cm4. One of them was 13.5 cm 5 and a second case was 15 cm.6
Atherosclerosis, hypertension, smoking, obstructive pulmonary diseases, familiar factors, inflammatory reactions, and chronic mucoid degenerations are the risk factors of aortic rupture in patients with abdominal aneurysm.7
Clinical and surgical techniques and management of ruptured huge AAAs may present many difficulties. It may proceed proximal the clamping over renal arteries or supraceliac during an emergency.8 However, single or two stage strategies may be required for a thoraco-abdominal incision. The proximal control can alternatively be the use of aortic occlusion balloon catheter inserted through.
Also the proximal sac control can be compressed towards the vertebral column. In addition, femoro-axillary cardiopulmonary bypass for abdominal aortic repair can be used. Veno-arterial extracorporeal membrane support can be performed immediately to protect against higher risk of bleeding, respiratory and renal failure.8 Aorto-caval fistula or repair caval wall bleeding can be achieved by suturing or ligating. To avoid a pulmonary embolism, repair with synthetic grafts can be chosen.
Especially, endovascular endostent techniques (EVAR) can be used in suitable cases. An appropriate landing zone may be necessary and a contralateral limb catheterization may be difficult. Also, EVAR hybrid approach and femoral crossover bypass can be performed. Blood loss may be controlled by using cell saver or endovascular techniques.
Finally, the number of the patients is limited and younger (than 59 years old) in our case, and this is one of the giant AAAs. Aneurysm was 15 cm in diameter and operated with a very high risk of mortality because of the rupture. We used finger compressing method to the vertebral column and also used Foley?s urinary catheter as endo-aortic balloon clamp inserted through to control the proximal neck. In our case, combined intensive care unit and hospital uneventful stay were 2 and 5 days, respectively.
In conclusion, for the treatment of ruptured abdominal aortic aneurysm requires more experience and have high mortality and morbidity rates. Timing of the operation (before rupture), perioperative bleeding is very important for decreasing the risk. Also, abdominal examination of the patient is important. Aneurysms can be detected simply by physical examination that can reduce the mortality and morbidity.
Acknowledgement
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the authorship or publication of this article.
Funding
The authors received no financial support for the research or authorship of this article.
References
- Schermerhornm L, Cronenwett J L. Abdominal aortic and iliac aneurysms. Vascular Surgery. Philadelphia, Pennsylvania, W:B: Saunders Company, 2005;(6) 1416-20.
- Vural H, et.al. Giant size abdominal aortic aneurysm repair using open proximal anastomosis under hypothermic circulatory arrest: a report of two cases. J Vasc Surg 2007; 46(2): 363-5.
- Choke E, et al. A review of biological factors implicated in abdominal aortic aneurysm rupture. Eur J Vasc Endovasc Surg, 2005; 30 (3): 227-44.
- D. Maras, et al. Giant Abdominal Aortic Aneurysms :Clinical and Technical Considerations. Acta Chir Belg, 2009; 109(3); 376-80.
- SchubertT F. Giant aneurysm of the abdominal aorta. Australas Radiol, 1995; 39(1): 58-60.
- Woolgar J. D., Robbs J. V. Giant abdominal aortic aneurysm secondary to intimomedial mucoid degeneration. Postgrad Med J, 2001; 77(914): 782.
- Cronenwett J, et al. Actuarial analysis of variables associated with the rupture of small abdominal aortic aneurysms. Surgery, 1985; 98(3): 472-83.
- Buket S, et al. Proximal clamping levels in abdominal aortic aneurysm surgery. Tex Heart Inst J, 1999; 26(4): 264-8.
|